
A Systematic Survey on Cybersickness in Virtual Environments


School of Electrical Engineering and Computer Science, University of North Dakota, Grand Forks, ND 58201, USA
*
Author to whom correspondence should be addressed.
Computers 2022, 11(4), 51; https://doi.org/10.3390/computers11040051
Submission received: 12 October 2021
/
Revised: 21 March 2022
/
Accepted: 24 March 2022
/
Published: 29 March 2022
Abstract
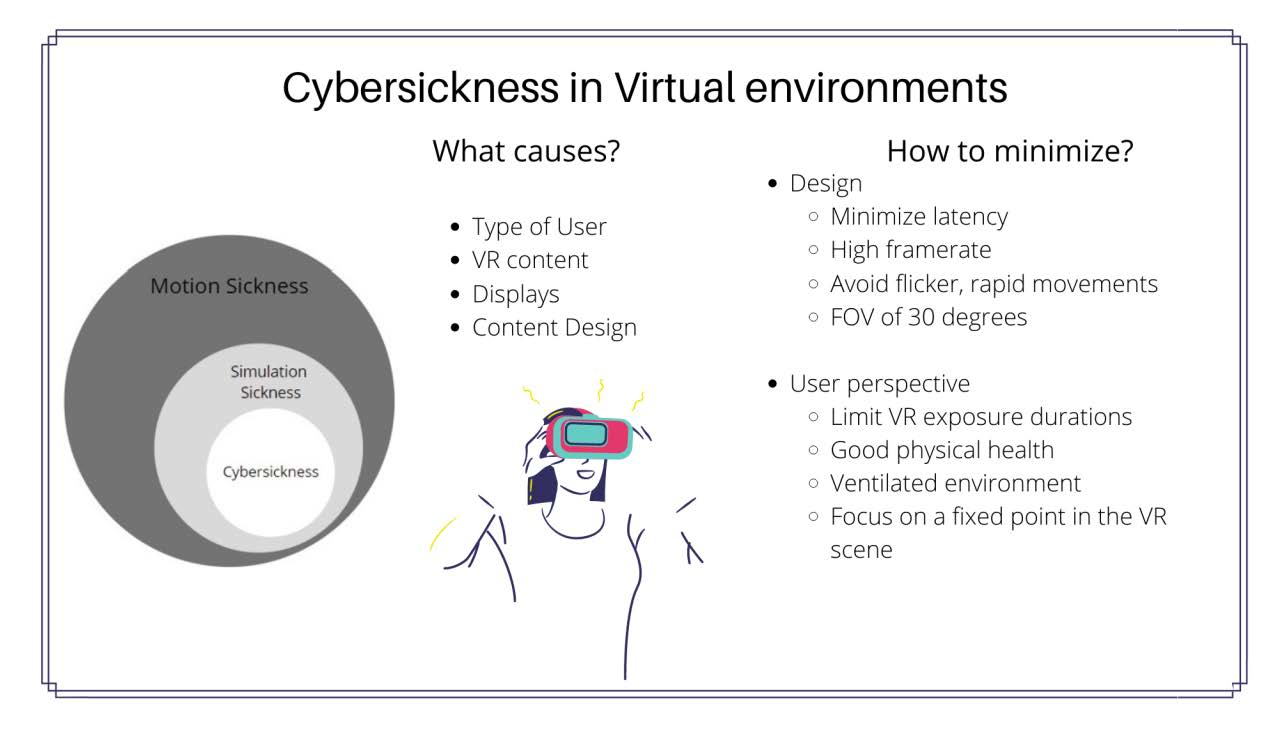
:Virtual reality (VR) is an emerging technology with a broad range of applications in training, entertainment, and business. To maximize the potentials of virtual reality as a medium, the unwelcome feeling of cybersickness needs to be minimized. Cybersickness is a type of simulation sickness that is experienced in virtual reality. It is a significant challenge for the usability of virtual reality systems. Even with advancements in virtual reality, the usability concerns are barriers for a wide-spread acceptance. Several factors (hardware, software, human) play a part towards a pleasant virtual reality experience. In this paper, we review the potential factors which cause sickness and minimize the usability of virtual reality systems. The reviewed scientific articles are mostly part of documents indexed in digital libraries. We review the best practices from a developer’s perspective and some of the safety measures a user must follow while using the virtual reality systems from existing research. Even after following some of the guidelines and best practices virtual reality environments do not guarantee a pleasant experience for users. Limited research in virtual reality environments towards requirements specification, design, and development for maximum usability and adaptability was the main motive for this work.

1. Introduction
Alternative reality creation and interaction requires a different set of capabilities. Modern developments in software and hardware technologies have unlocked new prospects for interactions. Virtual reality (VR) allows for three-dimensional visualization with immersive and interactive features [1]. A soaring interest in virtual reality (VR) technology has increased integration into numerous disciplines such as education, games, and training [2]. A report from artillery intelligence in 2021 states that approximately 23% of US households have access to a virtual reality headset [3]. A Goldman Sachs report on understanding the future of technologies predicts that VR and AR software will become a $35 billion industry by 2025 [4]. Advancements in VR technology have significant shortcomings. Virtual reality tools are known to have adverse physiological and psychological consequences, [5] such as simulation sickness, a type of motion sickness induced by mobile simulators without head tracking [6].
Cybersickness is a form of simulation sickness experienced when using head mounted displays (HMDs) and is a critical issue that needs to be addressed before virtual reality technology is widely accepted. The concept of cybersickness has existed since the early stages of VR system development. However, it was referred to as motion sickness. A combination of symptoms such as nausea, fatigue, headache, strain, postural instability, and vomiting define cybersickness [7], which is a possible consequence of the intense visual and motion cuing when experiencing a virtual environment [8]. Previous research states that approximately 20–80% of virtual reality users have experienced cybersickness or related discomfort at least once [9]. Cybersickness is measured through simulation sickness questionnaires and physiological measurements such as heart rate, postural sway, and galvanic skin response.
Usability, or ease of use, is essential when developing immersive VR applications. Fatigue, space limitation, predictability, and accessibility are usability issues associated with virtual reality content [10]. Cybersickness also limits the overall usability of a VR system [7]. Researchers that study virtual reality, human computer interaction (HCI), and organizations focused on VR have been thriving since they focus on minimizing cybersickness and improving the usability of virtual environments [11,12]. We have focused on simulation sickness in virtual reality environments for this review. Virtual reality offers remarkable opportunities for research and development. Minimizing cybersickness is vital for greater virtual reality application acceptance. Existing research on sickness in virtual reality systems focuses on individual aspects, such as causes, factors, relationships between factors, and cybersickness.
Cybersickness can be a result of software, hardware, or other environmental factors. The motivation for this work is to compile details on simulation sickness and its types, such as cybersickness; causes; theories that explain simulation sickness, such as poison theory and postural instability theory; factors causing simulation sickness; and guidelines on how to minimize or avoid these issues. The identified factors that contribute to simulation sickness are classified according to user, display type, VR content type, and virtual environment design. We have identified and grouped guidelines for users and virtual reality content developers. We attempt to offer insight into existing research on factors and guidelines aimed at minimizing simulation sickness.
2. Background
2.1. Virtual Reality
Virtual reality technology visualizes multi-dimensional (2D, 3D) content in perceptual space with immersive interactions [13] through a combination of computer graphics, image processing, sound, haptic systems, and advanced software and hardware. Human interactions with simulations provide fabricated feedback to sensory systems [14,15].
Multiple types of virtual reality exist based on the target display conditions. Desktop virtual reality, in which the virtual content is displayed on conventional desktop screens. These systems do not support sensory output and are simple VR applications. Fish tank virtual reality is a refined version of virtual reality that supports head tracking to improve presence in a virtual environment. These systems also use conventional monitors and do not support sensory output. Immersive virtual reality uses head-mounted displays (HMDs) to display multi-dimensional content, adjusting to stereoscopic views according to user movements. Table 1 summarizes the different types of VR based on the features and hardware used.
Immersion in a virtual reality system is a vital characteristic as the simulated content is user-centric. Humans visualize and interpret the environment around them in three dimensions (3D). This characteristic helps us adapt to the virtual world since it appears as a natural world [16]. Designing virtual reality systems based on human factors is said to have a sense of presence or immersion [17,18].
2.2. Usability
Usability, or the level of user satisfaction, is a quality attribute of any given system. This attribute combines quality components, such as learnability, efficiency, satisfaction, memorability, and errors [19]. Usability is achieving the goals of efficiency, effectiveness, and satisfaction in a specific context for the user of a product, service, or system, according to ISO 9241 [20].
Brian Shackel first introduced the concept of usability in 1986 as part of his research on human-computer interaction (HCI). Many other studies have backed the concept of usability in their research to support the development of effective, interactive, and efficient interfaces for the user. Usability can be determined by surveying users after they execute real tasks on a system and analyzing their feedback is known as usability testing, achieved by hard and soft methods [21]. The time to learn about the system, its ease of use, and errors made during system operation are detailed in both methods to examine the system’s usability [22,23].
2.2.1. Usability in Virtual Reality
Virtual reality experiences are a combination of interaction, immersion, and imagination. These are known as the three vertices of a virtual reality system [22]. Immersion is an essential aspect of a virtual reality system. Interactions in a VR system are 3-dimensional (3D), in contrast to conventional desktops. As humans visualize and interpret the world around them in three dimensions, 3D multi-modal interfaces facilitate adjustments to the virtual world. Designs based on human factors will have a higher sense of presence or immersion [17].
2.2.2. Issues
Exposure to virtual reality environments has varied effects on the user. The variations in the usability of immersive VR systems have effectively decreased with the swift techno- logical developments of HMDs. However, studies embracing advanced HMDs for research are minimal [24]. Usability is a crucial and intricate consideration when training older adults in virtual reality with non-immersive content. Usability should also be evaluated using surveys, interviews, and questionnaires during the development design and test phases [25]. Advanced research studies must address these critical issues to adapt VR environments effectively [26]. Virtual environment issues are classified into safety, direct, indirect, and social effects based on their impact area [26,27].
Direct effects in a virtual environment include multiple levels of user damage, such as macroscopic issues that lead to trauma or serious injury and microscopic issues that cause invisible damage. Indirect effects include the physiological consequences of over exposure to a VR environment at a functional level. Virtual reality system interactions depend on human senses, which is one of the main reasons virtual reality developers must understand the physiology of human senses and emotions if they want to build highly usable virtual systems. The data currently available from existing research is insufficient to assume that VR provokes violent social behavior [26].Users prone to light, motion, and sound sensitivity may have an uncomfortable virtual experience [27]. We have summarized the effects of a virtual reality system in Table 2 [28].
A VR experience might be unrealistic if the optical flow patterns are incorrect or the rendered scene lacks realism, even with a better understanding of human physiology [29]. Understanding the human ear and its ability to track audio sources is essential. Audio source intensity and frequency must be localized to help the user distinguish between different sounds in multi-dimensional audio. Haptic touch, a mechanical stimulation that mimics the human touch, enhances the usability and performance of VR. One known issue with haptic touch is that human skin adapts to it over time and skin sensitivity decreases. Modern technologies that involve human operations always need to ensure health and safety. Researchers often overlook the social implications of this technology; the severity and violence in VR games are concerns that must be addressed. Virtual actions may be provocative in the real world, and a lack of guidelines that gauge violent behavior and difficulties in re-creating relationships outside of laboratories are some of the challenges researchers face [26,27].
3. Systematic Review
The goal of this survey is to explore the physiological factors towards cybersickness and bring together some recommendations based on prior research. A systematic review was performed to gather information relevant to cybersickness, virtual reality, causes, and factors (Table 3).
Using the search term cybersickness in key research databases for journal and conference papers with just the term ‘cybersickness’ provided 6830 papers. A wide range of articles focused on cybersickness in various areas of virtual environments. The results also comprised of articles focusing on detection, prediction, and measurement of cybersickness with traditional and unconventional methods.
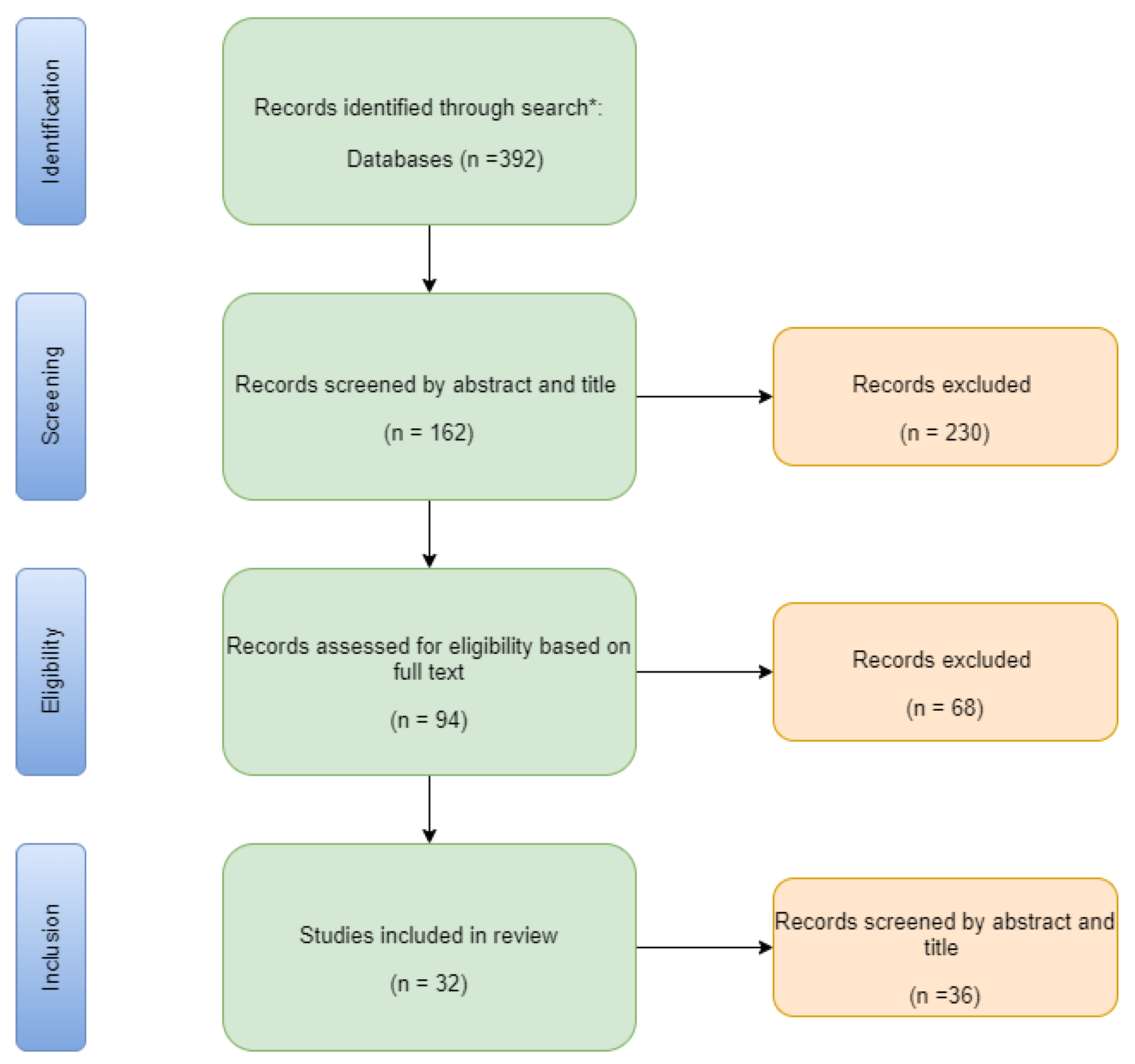
As the focus of the paper was towards theories, factors, and cybersickness as an issue in virtual reality, the results have been refined by adding the search terms such as factors contributing to cybersickness, cybersickness theories, and causes of cybersickness. The flowchart in Figure 1 shows the application of PRISMA approach for evaluating articles for the systematic review [30].
4. Simulation Sickness in Virtual Environments—Cybersickness
Virtual reality systems provide an immersive experience with the help of high-resolution displays, spatial sound, and interactive devices. However, interactive environments have shortcomings that contribute to physiological effects and threaten the usability of the virtual reality environment.
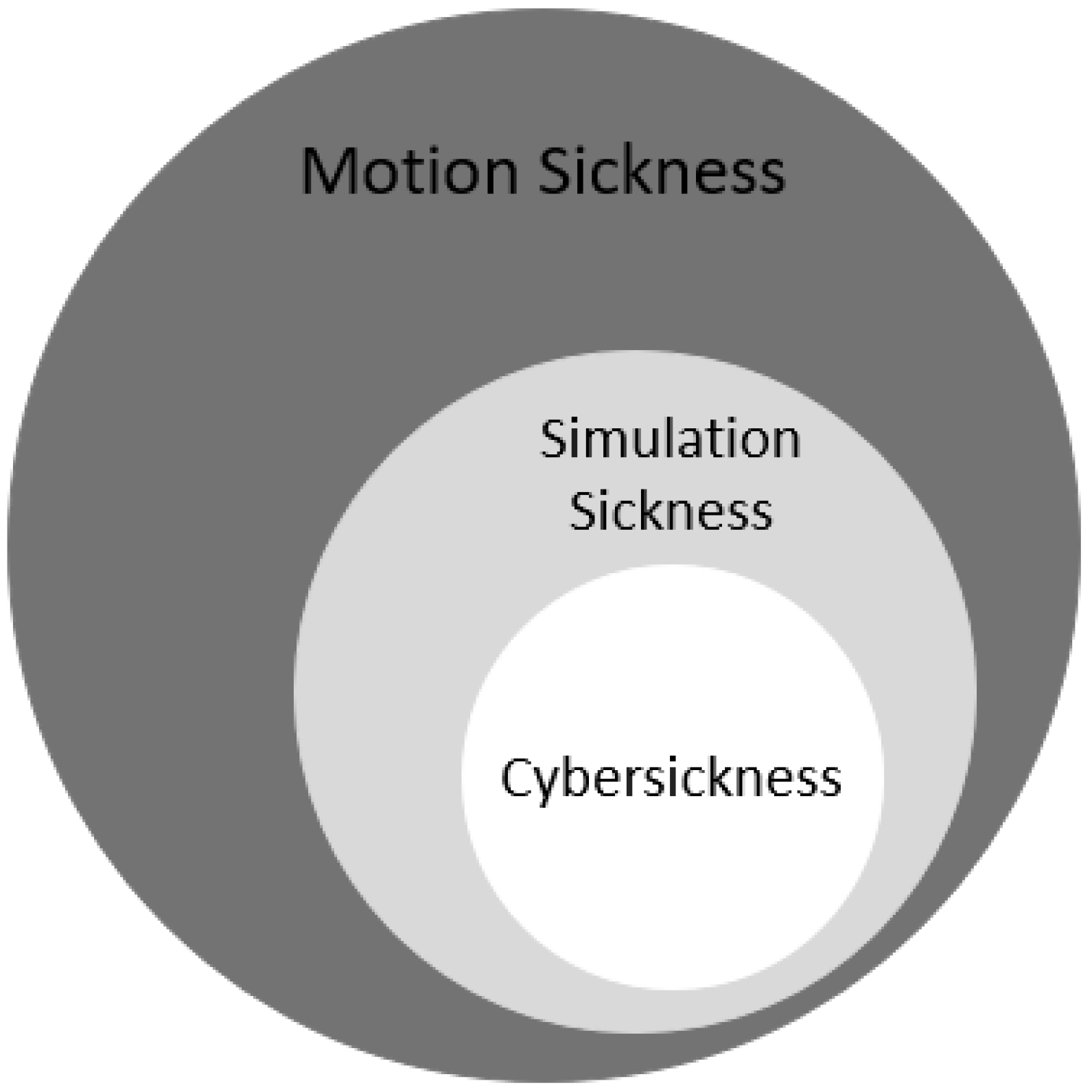
Simulation sickness is a condition that can result in headaches, dizziness, eye strain, disorientation, vertigo, loss of skin color, nausea, and vomiting. This condition, which can appear while using simulators or virtual reality devices, is comparable to motion sickness, though it is technically different. Figure 2. depicts the clear distinction between motion sickness, simulation sickness, and cybersickness.
Previous research, dating back to early 2000s, does not denote or consider advancements in virtual reality and other simulation technologies [32]. Another kind of sickness, more similar to simulation sickness or motion sickness is induced when using a VR system, denoted as virtual reality induced symptoms and effects (VRISE) [15], visually induced motion sickness (VIMS), or cybersickness [12].
Cybersickness is a significant issue that prevents the functional use of fully immersive virtual reality systems. It is a form of motion sickness and is one of the primary health and safety concerns of virtual environments, posing a severe threat to usability and performance [33]. Some of the issues associated with virtual reality systems are assumed to result from poor system design, including virtual scene and user control strategies, technical deficiencies such as image distortions, visual cues, and individual user susceptibility. Some human factors that limit performance also contribute to the reduced popularity of virtual reality systems [34].
4.1. Cause of Sickness—Theories
The occurrence of simulation sickness has been a topic of research since the early 19th century. The earliest theories addressing simulation sickness were based on cerebral anemia, which is deprived blood supply to the brain, or cerebral hyperemia, which is the congestion of blood in the brain and spinal cord. These studies advanced significantly during the post-World War II era. Vestibular and sensory conflict are some of the earliest theories that focus on simulation sickness [35]. Simulation sickness is the result of the difference between the information received by the vestibular and the visual systems in a virtual environment, according to sensory conflict theory [35]. There is a significant mismatch when the visual information specifies movement while the vestibular system indicates that the user is stationary due to the conflict between the sensory inputs, causing the user to experience simulation sickness. Postural instability theory states that extended periods of postural instability cause motion sickness symptoms, the level of which is directly proportional to the duration [36]. Poison theory states that the feeling of nausea caused by simulation sickness is the body’s response to the mismatch of visual and vestibular information. The body assumes it is suffering from food poisoning and triggers the sensation of the need to vomit, or similar sensations [37]. All of these theories, including eye movement, subjective vertical mismatch, and negative reinforcement models, describe the cause of motion sickness that occurs when using virtual reality systems. However, the most widely accepted is sensory conflict theory [34].
4.2. Cybersickness as a Usability Issue
Virtual reality creates an opportunity to visualize an altered three-dimensional world. However, it requires full sensory awareness for maximum effectiveness. Interactions and visual cues in virtual environments must be well designed to be as close to the real world as possible before VR is understood and adapted well. The extent to which the user feels present in the environment indicates its success. Therefore, usability issues will diminish the sense of presence in a virtual environment. Users will not be able to experience the reality of a virtual environment if they struggle to use the environment. D. Geszten et al. [38] suggests that presence and copresence should be the primary goals when designing VR environments and should be examined when evaluating the usability of these environments.
5. Factors Contributing to Cybersickness
Many potential factors contribute to simulation sickness in virtual environments, such as age, gender, calibration, experience, and application type. P.J Costello [5] has tabulated many of these factors based on the individual, simulator type, and task performed. These factors have a profound impact on the severity of cybersickness. The factors affecting virtual reality are classified according to user, design, display types, and type of VR content. Table 4, provides an overview of some of the factors that contribute to simulation sickness.
5.1. Users
5.1.1. Age
Cybersickness is primarily based on sensory conflict theory and postural in-stability theory. Literature suggests that younger people are more resistant to simulation sickness [32]. Vestibular perceptual threshold, the weakest stimulus detected, diminishes in humans after the age of 40, making them more susceptible to simulation sickness [39]. Era et al. reported that there were postural balance differences between young and middle-aged test participants. In addition, higher age groups experience diminished postural balance which may lead to sickness [40].
5.1.2. Gender
Simulation sickness may vary according to gender with the use of HMDs. Schafer et al. [41] studied the role of gender, technology, and their potential contribution towards simulation sickness. Using the data obtained from about 223 individuals (108 male and 115 female) they examined the levels of simulation sickness with regards to gender, sensory conflict, and improvements in VR technology. They concluded that women experienced a higher level of simulation sickness compared to men. Stanney et al. [42] conducted multiple experiments and found that females were equally susceptible to motion sickness, and it was due to the improper fit of the VR headset to inter-pupillary distance (distance between the center of one’s eyes). They also suggest a redesign to the VR headsets with alterable inter-pupillary distance to reduce the cybersickness in women.
5.1.3. Exposure
Stanney et al. [43] concluded that an increase in exposure time was directly proportional to the severity of adverse symptoms. Users vulnerable to motion sickness can experience approximately twice the intensity compared to non-susceptible individuals. Users who experience nausea during carnival rides can also expect unpleasant symptoms. Exposing an individual to virtual environments briefly and stopping the encounter before or while experiencing sickness then retrying in a day or two will help the user adapt to the virtual environment. Recurring exposure to virtual environments may lower or eliminate simulation sickness. However, using a virtual environment for longer durations is not recommended [32].
5.1.4. Control
User control and navigation are substantial contributing factors to simulation sickness since input devices, such as data gloves, keyboards, and mice, can be used to control the virtual environment. Greater environmental control may reduce illness and allow users to expect a reaction after an action is performed [15]. Saredakis et al. [44] observed that physical navigation, such as walking, reduces symptoms compared to navigating through controllers.
5.2. Displays
A difference in environments, such as desktop VR, large curved screen displays, or HMD’s can have a varied impact on the level of sickness [15].
5.2.1. Head Mounted Display (HMD)
Factors such as contrast, illumination, exposure duration, and working distance contribute to straining the visual system when working with head mounted displays. Approximately 60% of users reported symptoms such as visual strain, nausea, and headache, while 20% reported a reduction in binocular visual perception when using a stereoscopic HMD, such as EyePhone LX, in an immersive virtual environment for a ten-minute duration [45]. Similar symptoms were experienced by 61% of users after twenty minutes of exposure to immersive virtual content from a DVisor HMD [46]. Technical advancements in VR display hardware, comparing Oculus VR DK1 to Oculus VR DK2, for example, did not have a significant impact on decreased cybersickness [41]. Some symptoms are more likely to occur in virtual environments. However. sensory conflict contributes significantly to nausea and other symptoms. Body motion, head movement-initiated disorientation, and incorrect optical design resulted in strain-producing ocular symptoms. Recent contributions from Tong et al. [47] determined that HMD use caused a higher level of motion sickness compared to stereoscopic desktop displays. Some users enjoyed a higher level of immersion in an HMD. However, they could not sustain the experience for longer periods.
5.2.2. Large and Desktop Displays
Former investigations report that viewing time, viewing distance, and lighting may also contribute to simulation sickness [48,49]. The optimum viewing distance is 65 cm. Swindells et al. concluded that large displays improve a sense of presence, but they do not directly impact or induce simulation sickness [50].

{kind=link}
{kind=link}
{kind=link}
Table 4.
Factors contributing to simulation sickness.
| Factors | Type | Effects | References |
|---|---|---|---|
| User | Age | Younger and middle-aged people are more resistant to sickness than older adults | [39,40] |
| Gender | Females are more prone to motion sickness than Males | [41,42] | |
| Exposure to VR | Longer VR exposure durations are directly proportional to the severity of sickness. | [43] | |
| Control | Users navigating with virtual controls might experience higher levels of cybersickness than those who use physical navigation | [15,44] | |
| Display | Head-Mounted Displays | Produce high levels of cyber sickness. | [45,46] |
| Large displays | Do not directly impact or induce sick-ness | [48,49,50] | |
| Immersion VR Content | Non-immersive content triggers less simulation sickness. The reverse is also true | [51] | |
| Graphic Realism | Realistic graphic content can cause more simulation sickness. | [2] | |
| Field of view | Altering the FOV minimizes user discomfort. | [2,8] |
5.3. VR Content Type
5.3.1. Immersion
Guna et al. studied the impact of virtual content type on simulation sickness. They noticed that the type of video content, immersive vs. non-immersive, is a critical factor for virtual environment usability. Video content type influenced the contributor’s sensitivity to simulation sickness and physiology. Their conclusion was based on the results of a simulation sickness questionnaire and other physiological measures. The lowest simulation sickness questionnaire score was recorded for non-immersive virtual content displayed on a television screen, while the highest scores were reported on an HMD with immersive content [51].
5.3.2. Graphic Realism
Chang et al. investigated the results of rendering realistic scenes. Participants who experienced realistic graphic content were prone to a higher level of simulation sickness. The authors also suspect that a sensory discrepancy between the vestibular and visual systems may cause a higher level of discomfort [2].
5.3.3. Field of View
Field of view (FOV) is the maximum visual angle of the virtual environment display. It is the visual range of the virtual world through the HMD or other display device. Altering the FOV of a display manually or dynamically significantly reduces user discomfort during swift and rotating movements [2,8].
5.4. Design
The virtual reality (VR) environment is a rapidly emerging technique for simulating real-world applications. Examples of successful application domains include training, therapy, and design. Simulating realistic features that support a wide range of activities is difficult, even with recent developments. Designing and executing virtual environments with a high degree of similarity to the real world is a significant challenge since human interactions are highly associated with sensory information. Minimal training is needed for interacting when the simulated system is close to natural, which correlates well to the system’s usability. Sustaining realism in the simulated world has its benefits. However, if the virtual environment is far from real, there is a need for remarkable visual patterns based on the application environment. Virtual reality, by definition, comprises immersive environments that use multi-modal inputs, such as haptic, visual, and speech, and outputs, such as HMD’s and other displays, to create a maximum presence for the user. Designing complex virtual environments is a delicate task since it requires managing hardware, general user safety, and visual content that may cause disorientation or sickness. The design process for desktop VR environments is straightforward. However, the presence it draws is minimal and is less effective in tasks that include physical interaction [52].
6. Guidelines to Minimize Simulation Sickness
Hardware improvements improve the usability of virtual environments [53], and existing research suggests that some techniques used to achieve maximum usability can minimize simulation sickness [54]. Virtual reality hardware manufacturers, such as Oculus and HTC, have detailed design guidelines for content developers and hardware safety guidelines for users [55].
6.1. Design
It is impossible to have an ideal set of guidelines for any software system. However, we have summarized some critical ones from existing research, that must be considered when designing virtual environments to reduce simulation sickness symptoms.
6.1.1. Latency and Frame Rate
Latency is the delay between the user and visual reaction in a virtual environment display. Frame rate is a measure of how quickly the frames pass through the rendering pipeline. A drop in frame rate can occur in a VR application with complex graphics. There is a high chance of experiencing simulation sickness if the latency between the user input and virtual content output is high [54]. The minimum recommended latency is 20 milliseconds: anything higher than 46 milliseconds can induce motion sickness. Companies such as Oculus, Sony, and Steam emphasize the importance of virtual content with low latency, responsiveness, and high frame rates for higher virtual content quality [32,56].
6.1.2. Movement
The VR’s user does not always control character movements. This movement unavailability can cause serious issues. Therefore, movement in a virtual environment should be realistic to match sensory expectations. Inappropriate movements, such as fast tilting, rolling, and waveform motion, should be avoided. Examples of these inappropriate movements include gun sway, head bob, and going up and down stairs. Porcino et al. [54] suggest that including movements based on jumps instead of continuous walks may minimize sickness. Uncontrolled user movement outputs should be limited, such as flipping, falling, or zoom transitions [32].
6.1.3. Flicker
Flicker is the brightness fluctuation on video displays and can cause sickness in a VR environment. This fluctuation is visually disturbing and affects the health of the user’s eyes. The user is more likely to experience flicker in the edges of the screen when using larger displays. Flicker avoidance is essential for HMDs with a brighter screen and high refresh rate [2,32].
6.1.4. Rapid Changes in Acceleration and Deceleration
A vital factor in virtual environment discomfort is accelerated movement. Sensory conflicts that cause discrepancies occur due to sudden increased or decreased acceleration. Therefore, increasing or decreasing acceleration slowly would result in a pleasant user experience [54]. Rapidly zoomed movements should also be avoided, such as when the visual cones move faster than expected when a user’s view is zoomed in [32].
6.1.5. Sensory Support
A user might experience higher VR immersion and expect relevant vestibular in- formation after exposure to strong illusions. The system can cause motion sickness if the VR system cannot provide suitable sensory input [8]. Therefore, designing a logical environment in which the players can focus and bind to is essential. The user interface elements should be fixed rather than floating, creating an environment with a clear, steady horizon and reference points that users can focus on to minimize sickness. A world with imbalanced or changing backgrounds should be avoided. Designing a virtual world that supports human sensory systems is ideal [32].
6.1.6. Field of View (FOV)
A wide field of view (FOV) in a display may increase immersion in the virtual environment. Narrow field of views may affect the presence in the virtual environment, which is an important characteristic. Displays with a broader field of view increase the occurrence of simulation sickness more than those with a narrow field of view [8]. The edges of a display with a narrow field of view reduce the simulation view, which reduces the feeling of movement [54].
6.1.7. Length of Exposure
Longer duration of exposure can increase discomfort levels. Applications should be designed to support shorter exposure duration to allow users to pause, rest, and continue later. Optimal application design would include automatic suggestions to the user that encourage regular breaks [54]. There should be provisions for the user to come back and continue from the same stage in the application if they are getting sick and leave the session. Therefore, shorter exposure sessions are beneficial [2,32].
Table 5, presents an overview of some of the design practices from the researchers and VR development organizations. Most of these practices have been suggested as individual standard work. However, they have not been collectively tested to obtain better usability results.
6.2. User
Every user is unique and has individual characteristics and those play a vital role in the way they experience cybersickness. Based on the existing research and some guidelines provided by virtual reality hardware and software organizations users can minimize cybersickness by following best practices.
6.2.1. Duration
6.2.2. Focus
Human brains focus on a fixed point in space outside of a virtual environment. VR confuses the brain since the fixed point in space looks farther, but the image on the headset screen is immediately in front of the eyes. Focusing on an object on the VR scene’s horizon may reduce sickness symptoms [32,57].
6.2.3. Environment
Cybersickness symptoms strengthen in surroundings with high temperature and poor ventilation. Good airflow and ventilation can prevent nausea or support recovery after experiencing dizziness [32].
6.2.4. Physical Health
All of the user’s senses must be optimal to achieve an elevated presence level. Users should be physically healthy and have good balance for the best virtual reality experience. If a user has a cold, headache, or hangover, it is better to avoid a virtual environment since their symptoms may worsen [54]. The guidelines mentioned above will only minimize simulation sickness symptoms and improve the usability of the VR systems. These suggestions will not eliminate the symptoms [32,54]. In Table 6, a combination of guidelines is tabulated.
7. Cybersickness Varies by Age and Gender
Cybersickness varies with gender, age, exposure to VR, and the type of VR content. An empirical study has been conducted to verify the previous research conclusions that age, gender, experience with virtual reality content and other demographic features influence cybersickness. The online survey (https://und.qualtrics.com/jfe/form/SV 9ppzZX7qGwc4Rp4) (accessed on 15 March 2022) approved by the Institutional review board (IRB0003225) at the University of North Dakota intended to collect data on the users’ experiences with virtual reality and cybersickness. Preliminary results suggest that there is a correlation in between age, gender, experience with virtual reality content and cybersickness.
8. Conclusions
Virtual reality has the potential to transform entertainment, gaming, training, and many other industries. VR is still not accepted by a vast audience due to the existing sickness and discomfort, regardless of efforts made by multiple research and development organizations. This study is an extension of our earlier work, which examined the usability and performance evaluations of virtual environments. We have examined cybersickness severity and determined that human factors, VR content, and hardware trigger sickness in virtual environments. Cybersickness levels also vary with the type of setup. Quality attributes for virtual reality systems contribute a lot to the pleasant experiences, identifying the same from distinct audiences that are associated with virtual reality systems would benefit and boost the adaptability of the virtual reality systems must be identified. We have compiled some guidelines and best practices from existing research for virtual content developers and users to minimize sickness and improve the virtual environment experience. However, there is a need for a standardized development model to specify requirements, design, and develop virtual reality applications that result in maximum adaptability.
9. Future Work
We hope this research contributes to the users who suffer from cybersickness in virtual reality environments in helping them improve their user experience. One future direction is to employ a series of guidelines and verify their effectiveness in minimizing cybersickness and to employ a focused approach to compare virtual content with different levels of immersion on various HMDs.
Author Contributions
A.N.R.C. conceptualized and identified the need for a combined guidelines and best practices for minimizing cybersickness in virtual environments. In this work, A.N.R.C. wrote the paper and carried out the online empirical study needed to verify the previous research claims supported by H.R. The manuscript was improved based on feedback and proofreading from F.E.J. and H.R. All authors have read and agreed to the published version of the manuscript.
Funding
This review research did not receive any external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of University of North Dakota (IRB0003225, 07 June 2021) for studies involving humans in the Exempt 2 category.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study before completing the survey online.
Data Availability Statement
Not applicable.
Conflicts of Interest
There are no conflict of interest to declare.
Abbreviations
The following abbreviations are used in this manuscript:
| VR | Virtual reality |
| HMD | Head-mounted display |
References
- Keil, J.; Edler, D.; O’Meara, D.; Korte, A.; Dickmann, F. Effects of Virtual Reality Locomotion Techniques on Distance Estimations. ISPRS Int. J. Geo-Inf. 2021, 10, 150. [Google Scholar] [CrossRef]
- Chang, E.; Kim, H.T.; Yoo, B. Virtual Reality Sickness: A Review of Causes and Measurements. Int. J. Hum.-Comput. Interact. 2020, 36, 1658–1682. [Google Scholar] [CrossRef]
- AR Insider. New Report: 19 of U.S. Adults Have Tried VR; AR Insider. 2020. Available online: https://arinsider.co/2020/05/20/new-report-19-of-u-s-adults-have-tried-vr (accessed on 10 October 2021).
- Bellini, H.; Chen, W.; Sugiyama, M.; Shin, M.; Alam, S.; Takayama, D. Virtual & Augmented Reality: Understanding the Race for the Next Computing Platform (Goldman Sachs). Equity Res. 2016. Available online: https://www.goldmansachs.com/insights/pages/technology-driving-innovation-folder/virtual-and-augmented-reality/report.pdf (accessed on 10 October 2021).
- Nichols, S.; Patel, H. Health and safety implications of virtual reality: A review of empirical evidence. Appl. Ergon. 2002, 33, 251–271. [Google Scholar] [CrossRef]
- Dużmańska, N.; Strojny, P.; Strojny, A. Can Simulator Sickness Be Avoided? A Review on Temporal Aspects of Simulator Sickness. Front. Psychol. 2018, 9, 2132. [Google Scholar] [CrossRef]
- Stauffert, J.-P.; Niebling, F.; Latoschik, M.E. Latency and Cybersickness: Impact, Causes, and Measures. A Review. Front. Virtual Real. 2020, 1, 31. [Google Scholar] [CrossRef]
- Kim, Y.Y.; Kim, E.N.; Park, M.J.; Park, K.S.; Ko, H.D.; Kim, H.T. The Application of Biosignal Feedback for Reducing Cybersickness from Exposure to a Virtual Environment. Presence Teleoperators Virtual Environ. 2008, 17, 1–16. [Google Scholar] [CrossRef]
- Kim, H.; Kim, D.J.; Chung, W.H.; Park, K.A.; Kim, J.D.; Kim, D.; Kim, K.; Jeon, H.J. Clinical predictors of cybersickness in virtual re-ality (VR) among highly stressed people. Sci. Rep. 2021, 11, 1–11. [Google Scholar]
- Comfort and Usability: Oculus Developers; Oculus: Menlo Park, CA, USA, 2021; Available online: https://developer.oculus.com/resources/locomotion-comfort-usability/ (accessed on 10 October 2021).
- Al Zayer, M. Universal Usability of Virtual Reality. Ph.D. Thesis, University of Nevada, Reno, Nevada, 2019. [Google Scholar]
- McHugh, N. Measuring and Minimizing Cybersickness in Virtual Reality. Master’s Thesis, University of Canterbury, Christchurch, NZ, USA, 2019. [Google Scholar]
- Mazuryk, T.; Gervautz, M. Virtual Reality-History, Applications, Technology and Future; Institute of Computer Graphics, Vienna University of Technology, Austria. 1996. Available online: https://www.cg.tuwien.ac.at/research/publications/1996/mazuryk-1996-VRH/TR-186-2-96-06Paper.pdf (accessed on 10 October 2021).
- Bamodu, O.; Ye, X.M. Virtual reality and virtual reality system components. Advanced materials research. Trans. Tech. Publ. 2013, 765, 1169–1172. [Google Scholar]
- Sharples, S.; Cobb, S.; Moody, A.; Wilson, J.R. Virtual reality induced symptoms and effects (VRISE): Comparison of head mounted display (HMD), desktop and projection display systems. Displays 2008, 29, 58–69. [Google Scholar] [CrossRef]
- El Jamiy, F.; Marsh, R. Survey on depth perception in head mounted displays: Distance estimation in virtual reality, augmented reality, and mixed reality. IET Image Process. 2019, 13, 707–712. [Google Scholar] [CrossRef]
- 3D Multimodal Interaction Design. In Designing Virtual Reality Systems The Structured Approach; Springer: London, UK, 2005; pp. 122–152. [CrossRef]
- Jamiy, F.E.; Marsh, R. Distance Estimation In Virtual Reality And Augmented Reality: A Survey. In Proceedings of the 2019 IEEE International Conference on Electro Information Technology (EIT), Brookings, SD, USA, 20–22 May 2019; pp. 63–68. [Google Scholar] [CrossRef]
- Nielsen, J. Usability 101: Introduction to Usability; Nielsen Norman Group: Fremont, CA, USA, 2012; Available online: https://www.nngroup.com/articles/usability-101-introduction-to-usability/ (accessed on 10 October 2021).
- ISO. Ergonomics of Human-System Interaction—Part 210: Human-Centred Design for Interactive Systems; International Organization for Standardization, 2019. Available online: https://www.iso.org/obp/ui/#iso:std:iso:9241:-210:ed-2:v1:en (accessed on 10 October 2021).
- Anandhan, A.; Dhandapani, S.; Reza, H.; Namasivayam, K. Web Usability Testing—CARE Methodology. In Proceedings of the Third International Conference on Information Technology: New Generations (ITNG’06), Las Vegas, NV, USA, 10–12 April 2006; pp. 495–500. [Google Scholar]
- Falcao, C.; Soares, M. Applications of Haptic Devices & Virtual Reality in Consumer Products Usability Evaluation; AHFE International (USA): Krakow, Poland, 2014; pp. 377–383. [Google Scholar] [CrossRef]
- Galster, M.; Widmer, A. Quality Attributes in Medical Planning and Simulation Systems. In Relating System Quality and Software Architecture; Elsevier: Amsterdam, The Netherlands, 2014; pp. 287–289. [Google Scholar]
- Pallavicini, F.; Pepe, A.; Minissi, M.E. Gaming in Virtual Reality: What Changes in Terms of Usability, Emotional Response and Sense of Presence Compared to Non-Immersive Video Games? Simul. Gaming 2019, 50, 136–159. [Google Scholar] [CrossRef]
- Tuena, C.; Pedroli, E.; Trimarchi, P.D.; Gallucci, A.; Chiappini, M.; Goulene, K.; Gaggioli, A.; Riva, G.; Lattanzio, F.; Giunco, F.; et al. Usability Issues of Clinical and Research Applications of Virtual Reality in Older People: A Systematic Review. Front. Hum. Neurosci. 2020, 14, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanney, K.M.; Mourant, R.R.; Kennedy, R.S. Human Factors Issues in Virtual Environments: A Review of the Literature. Presence 1998, 7, 327–351. [Google Scholar] [CrossRef]
- Viirre, E.; Bush, D. Direct effects of virtual environments on users. In Handbook of Virtual Environments; CRC Press: Boca Raton, FL, USA, 2002; pp. 581–588. [Google Scholar]
- Ramaseri Chandra, A.N.; El Jamiy, F.; Reza, H. A Review on Usability and Performance Evaluation in Virtual Reality Systems. In Proceedings of the 2019 International Conference on Computational Science and Computational Intelligence (CSCI), Las Vegas, NV, USA, 5–7 December 2019; pp. 1107–1114. [Google Scholar] [CrossRef]
- El Jamiy, F.; Ramaseri Chandra, A.N.; Marsh, R. Distance Accuracy of Real Environments in Virtual Reality Head-Mounted Displays. In Proceedings of the 2020 IEEE International Conference on Electro Information Technology (EIT), Chicago, IL, USA, 31 July–1 August 2020; pp. 281–287. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Bos, J. Motion Perception and Sickness, Eye Movevements and Human Performance, Jeltebos.info, 11 May 2017. Available online: https://www.jeltebos.info/perception_sickness.htm (accessed on 10 October 2021).
- Lewis-Evans, B. Simulation Sickness and VR—What Is It, and What Can Developers and Players Do to Reduce It? Game Developer. 2014. Available online: https://www.gamedeveloper.com/design/simulation-sickness-and-vr---what-is-it-and-what-can-developers-and-players-do-to-reduce-it- (accessed on 10 October 2021).
- Howarth, P.; Costello, P. Studies into the visual effects of immersion in virtual environments. Prod. Under HSE Res. Contract 1996, 3181, R53. [Google Scholar]
- Stanney, K.M.; Kennedy, R.S. Simulation Sickness; Raton, B., Ed.; CRC Press: Boca Raton, FL, USA, 2010. [Google Scholar]
- Reason, J.T.; Brand, J.J. Motion Sickness; Academic Press: Cambridge, MA, USA, 1975. [Google Scholar]
- Riccio, G.E.; Stoffregen, T.A. An ecological Theory of Motion Sickness and Postural Instability. Ecol. Psychol. 1991, 3, 195–240. [Google Scholar] [CrossRef]
- Treisman, M. Motion Sickness: An Evolutionary Hypothesis. Science 1977, 197, 493–495. [Google Scholar] [CrossRef]
- Geszten, D.; Komlódi, A.; Hercegfi, K.; Hámornik, B.; Young, A.; Köles, M.; Lutters, W.G. A Content-Analysis Approach For Exploring Usability Problems in a Collaborative Virtual Environment; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Rey, M.C.B.; Clark, T.K.; Wang, W.; Leeder, T.; Bian, Y.; Merfeld, D.M. Vestibular Perceptual Thresholds Increase above the Age of 40. Front. Neurol. 2016, 7, 162. [Google Scholar] [CrossRef]
- Era, P.; Sainio, P.; Koskinen, S.; Haavisto, P.; Vaara, M.; Aromaa, A. Postural Balance in a Random Sample of 7979 Subjects Aged 30 Years and Over. Gerontology 2006, 52, 204–213. [Google Scholar] [CrossRef]
- Shafer, D.M.; Carbonara, C.P.; Korpi, M.F. Modern virtual reality technology: Cybersickness, sense of presence, and gender. Media Psychol. Rev. 2017, 11, 1. [Google Scholar]
- Stanney, K.; Fidopiastis, C.; Foster, L. Virtual Reality Is Sexist: But It Does Not Have to Be. Front. Robot. AI 2020, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanney, K.M.; Hale, K.S.; Nahmens, I.; Kennedy, R.S. What to Expect from Immersive Virtual Environment Exposure: Influences of Gender, Body Mass Index, and Past Experience. Hum. Factors J. Hum. Factors Ergon. Soc. 2003, 45, 504–520. [Google Scholar] [CrossRef] [PubMed]
- Saredakis, D.; Szpak, A.; Birckhead, B.; Keage, H.A.D.; Rizzo, A.; Loetscher, T. Factors Associated With Virtual Reality Sickness in Head-Mounted Displays: A Systematic Review and Meta-Analysis. Front. Hum. Neurosci. 2020, 14, 96. [Google Scholar] [CrossRef] [Green Version]
- Mon-Williams, M.; Warm, J.P.; Rushton, S. Binocular vision in a virtual world: Visual deficits following the wearing of a head-mounted display. Ophthalmic Physiol. Opt. 1993, 13, 387–391. [Google Scholar] [CrossRef]
- Regan, E.C.; Price, K.R. The frequency of occurrence and severity of side-effects of immersion virtual reality. Aviat. Space Environ. Med. 1994, 65, 527–530. [Google Scholar]
- Tong, X.; Gromala, D.; Gupta, D.; Squire, P. Usability Comparisons of Head-Mounted vs. Stereoscopic Desktop Displays in a Virtual Reality Environment with Pain Patients. Stud. Health Technol. Inform. 2016, 220, 424–431. [Google Scholar]
- Taptagaporn, S.; Saito, S. How display polarity and lighting conditions affect the pupil size of VDT operators. Ergonomics 1990, 33, 201–208. [Google Scholar] [CrossRef]
- Dillon, T.W.; Emurian, H.H. Some factors affecting reports of visual fatigue resulting from use of a VDU. Comput. Hum. Behav. 1996, 12, 49–59. [Google Scholar] [CrossRef]
- Swindells, C.; Po, B.A.; Hajshirmohammadi, I.; Corrie, B.; Dill, J.C.; Fisher, B.D.; Booth, K.S. Comparing CAVE, wall, and desktop displays for navigation and wayfinding in complex 3D models. In Proceedings of the Computer Graphics International, Crete, Greece, 11–14 June 2004; pp. 420–427. [Google Scholar] [CrossRef]
- Guna, J.; Geršak, G.; Humar, I.; Krebl, M.; Orel, M.; Lu, H.; Pogačnik, M. Virtual reality sickness and challenges behind different technology and content settings. Mob. Netw. Appl. 2020, 25, 1436–1445. [Google Scholar] [CrossRef]
- Rosson, M.B.; Carroll, J.M. Usability Engineering: Scenario-Based Development of Human-Computer Interaction; Morgan Kaufmann: San Francisco, CA, USA, 2002; pp. 326–329. [Google Scholar]
- Terzić, K.; Hansard, M. Methods for reducing visual discomfort in stereoscopic 3D: A review. Signal Process. Image Commun. 2016, 47, 402–416. [Google Scholar] [CrossRef] [Green Version]
- Porcino, T.M.; Clua, E.; Trevisan, D.; Vasconcelos, C.N.; Valente, L. Minimizing cyber sickness in head mounted display systems: Design guidelines and applications. In Proceedings of the 2017 IEEE 5th International Conference on Serious Games and Applications for Health (SeGAH), Perth, WA, USA, 2–4 April 2017; pp. 1–6. [Google Scholar] [CrossRef] [Green Version]
- Introduction to Best Practices; Oculus: Menlo Park, CA, USA, 2020; Available online: https://developer.oculus.com/design/latest/concepts/book-bp/?locale=en_US (accessed on 10 October 2021).
- Raaen, K.; Kjellmo, I. Measuring Latency in Virtual Reality Systems. In Entertainment Computing—ICEC 2015; Chorianopoulos, K., Divitini, M., Baalsrud Hauge, J., Jaccheri, L., Malaka, R., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 457–462. [Google Scholar]
- Bles, W.; Wertheim, A. Appropriate Use of Virtual Environments to Minimise Motion Sickness. Hum. Factors Res. Inst Tno Soesterb. 2001. Available online: https://www.researchgate.net/publication/235020673_Appropriate_Use_of_Virtual_Environments_to_Minimise_Motion_Sickness (accessed on 10 October 2021).
Figure 1.
Article inclusion flow chart using PRISMA approach. * the results have been refined by adding the search terms such as factors contributing to cybersickness, cybersickness theories, and causes of cybersickness.
Figure 1.
Article inclusion flow chart using PRISMA approach. * the results have been refined by adding the search terms such as factors contributing to cybersickness, cybersickness theories, and causes of cybersickness.

Figure 2.
An overview of sickness types [31].
Figure 2.
An overview of sickness types [31].

Table 1.
Types of virtual reality [13].
Table 1.
Types of virtual reality [13].
| Type | Hardware | Sensory Support |
|---|---|---|
| Desktop | Conventional monitors | No |
| Fish tank | Conventional monitor + LCD shutter glasses | No |
| Immersive | Head mounted displays | Yes |
Table 2.
Types of effects in virtual reality environments [28].
Table 2.
Types of effects in virtual reality environments [28].
| Effect Type | Description | Example | References |
|---|---|---|---|
| Direct or Physical | Impact the human body targeting any individual tissue. | Hygiene, Injury | [5] |
| Indirect or Physiological | The physiological consequence of overexposure to a VR environment at a functional level. | Cybersickness, Postural instability | [26] |
| Safety | Safety needs to be a priority in a VR environment | Eye strain, Trauma. | [5,26] |
| Social or Psychological | Behavior issues | [25] |
Table 3.
Article search sources.
| Article Databases | IEEE Xplore, ACM Digital Library, Google Scholar |
| Article types | Journals, Conference paper, and Books |
| Search terms | Virtual Reality, Cybersickness, Factors, Causes |
Table 5.
Design and development guidelines.
| Guideline | Ideal | References |
|---|---|---|
| Latency | Low latency (less than 20 ms) | [32,54] |
| Frame rate | High | [32,56] |
| Movement | Realistic movements, Avoid involuntary | [32,54] |
| Flicker | Avoid or minimize | [2] |
| Field of view FOV | Narrow the better (This may vary with display type) | [57] |
| Rapid acceleration and deceleration | Avoid or minimize | [32,54] |
| Sensory System | Design to compliment the human senses | [8] |
| Shorter sessions of play | Design to support | [52,54] |
Table 6.
Best practices for users.
| Guideline | Ideal | References |
|---|---|---|
| Duration | Experience in shorter sessions or taking frequent breaks | [32,55] |
| Focus | Focusing on a rigid distant object on the horizon | [32,57] |
| Environment | High temperatures should be avoided, need good airflow and ventilation | [32] |
| Physical Health | User should be healthy and have good balance | [32,54] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ramaseri Chandra, A.N.; El Jamiy, F.; Reza, H. A Systematic Survey on Cybersickness in Virtual Environments. Computers 2022, 11, 51. https://doi.org/10.3390/computers11040051
AMA Style
Ramaseri Chandra AN, El Jamiy F, Reza H. A Systematic Survey on Cybersickness in Virtual Environments. Computers. 2022; 11(4):51. https://doi.org/10.3390/computers11040051
Chicago/Turabian StyleRamaseri Chandra, Ananth N., Fatima El Jamiy, and Hassan Reza. 2022. "A Systematic Survey on Cybersickness in Virtual Environments" Computers 11, no. 4: 51. https://doi.org/10.3390/computers11040051
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.