1. Introduction
Children with developmental language disorder (DLD) have difficulty using and understanding language. The estimated prevalence rate of DLD in kindergarten children is 7% [
1]. DLD impacts overall development and can have adverse effects on children’s well-being, school success, friendships, and employment [
2,
3,
4]. Speech and language therapy is the most common treatment for children with DLD. Via behavioral intervention, speech and language pathologists (SLPs) stimulate children’s language skills and teach them language learning strategies. The SLP will create opportunities for the child to practice the target skills while enjoying motivating toys and activities that are relevant to the child’s interest. Through joint attention, the child is facilitated to make associations between linguistic symbols and an item or event. Interaction occurs naturally, and target items can easily be repeated frequently. Motivation is an important factor, as it directs behavior toward particular goals, increases the time on a task, and enhances cognitive processing. At present, the most frequently used motivational toy children use by themselves is a game on a mobile device [
5]. It would therefore be interesting to know whether tablet games could be deployed effectively in speech and language therapy for children.
Interactive devices such as tablets have very rapidly found their way into today’s families and are among the most frequently used mobile devices among children. A report from Common Sense Media [
6] showed that 98% of homes in the United States with children under the age of 8 years had at least 1 mobile device such as a tablet, smartphone, e-reader, or gaming console. Kabali et al. [
7] used the same Common Sense survey for a study on 0–4-year-old children from low-income families. The study revealed that almost all children (96.6%) used mobile devices, and most started using them before the age of 1 year. At 2 years old, most children used a device daily and spent comparable screen time on television and mobile devices. Most 3- and 4-year-olds used devices without help, and one third engaged in media multitasking [
7]. A more recent study reported that 85% of Dutch children in primary education play video games on portable media, with 38% playing games daily and boys doing so more than girls [
5].
The advantages of tablets with touch screens over traditional personal computers are their multisensory character and more direct interaction with the user (Jesus et al., 2019). Moreover, tablets are handy devices because they are flat and lightweight with built-in audio and video, which makes them easy to handle and employ in an interactive therapy setting with children. Learning via these devices can be very motivating for children, and there is growing evidence that they can be beneficial to the acquisition of language and literacy in kindergarten and preschool children and support storybook comprehension in 2- and 3-year olds [
8,
9].
The almost universal adoption of interactive tablets by children and their potential to support learning have resulted in an increasing interest in using tablets and games in speech and language therapy. The Dutch SLPs we consulted to validate our research question recognize that for most children, gaming is fun, and it would be interesting to see if games can be added to the set of therapy materials in a meaningful way. However, they had mixed feelings and also expressed concerns that tablet games restrict the use of language-facilitating techniques and language interaction between the SLP and child and that tablet games might be too distracting. To date, little is known about if tablet games in therapy have a positive effect on the language learning outcomes of children with language needs. Trials with computer training often describe the effects of computer-based speech therapy with computer tasks that are developed for practicing at home. This approach is also known as ‘the virtual speech therapist’ [
10,
11]. A recent study on game-supported therapy showed a positive impact from using games on the motivation and satisfaction of children with speech and language disorders from 3 to 12 years old [
12,
13]. We think that the use of digital entertainment games corresponds to the way most SLPs work, as they often do not use specifically designed therapy material but creatively adapt broadly available toys and play materials to cover multiple treatment goals. An additional advantage of using entertainment games in therapy is that these games are accessible for parents, as they are often available either for free or at a low cost and therefore might easily be used to practice at home.
Our study aims to test whether tablet games can be used as effectively as traditional play material in therapy for children with DLD. Children are motivated to play tablet games, and we know that young children learn content and build vocabulary from interaction with peers and adults. Similar to working with traditional material, the SLP and child will engage in the tablet activities together. They will talk about the content, and the SLP will provide help when the child needs support. Therefore, our hypothesis is that vocabulary intervention with tablet games is as effective as standard intervention with traditional play materials. To test our hypothesis, we compared the number of new words children with DLD learned in two experimental intervention conditions with SLPs using either tablet games or real objects (toys) as materials. We chose enhancing vocabulary as the therapy goal because (1) many children with DLD experience problems in word learning [
14], (2) vocabulary training is used frequently in speech and language therapy, (3) vocabulary training is known to be effective [
15], and (4) vocabulary training often involves symbolic play in which tablet games or real play objects can be used.
2. Materials and Method
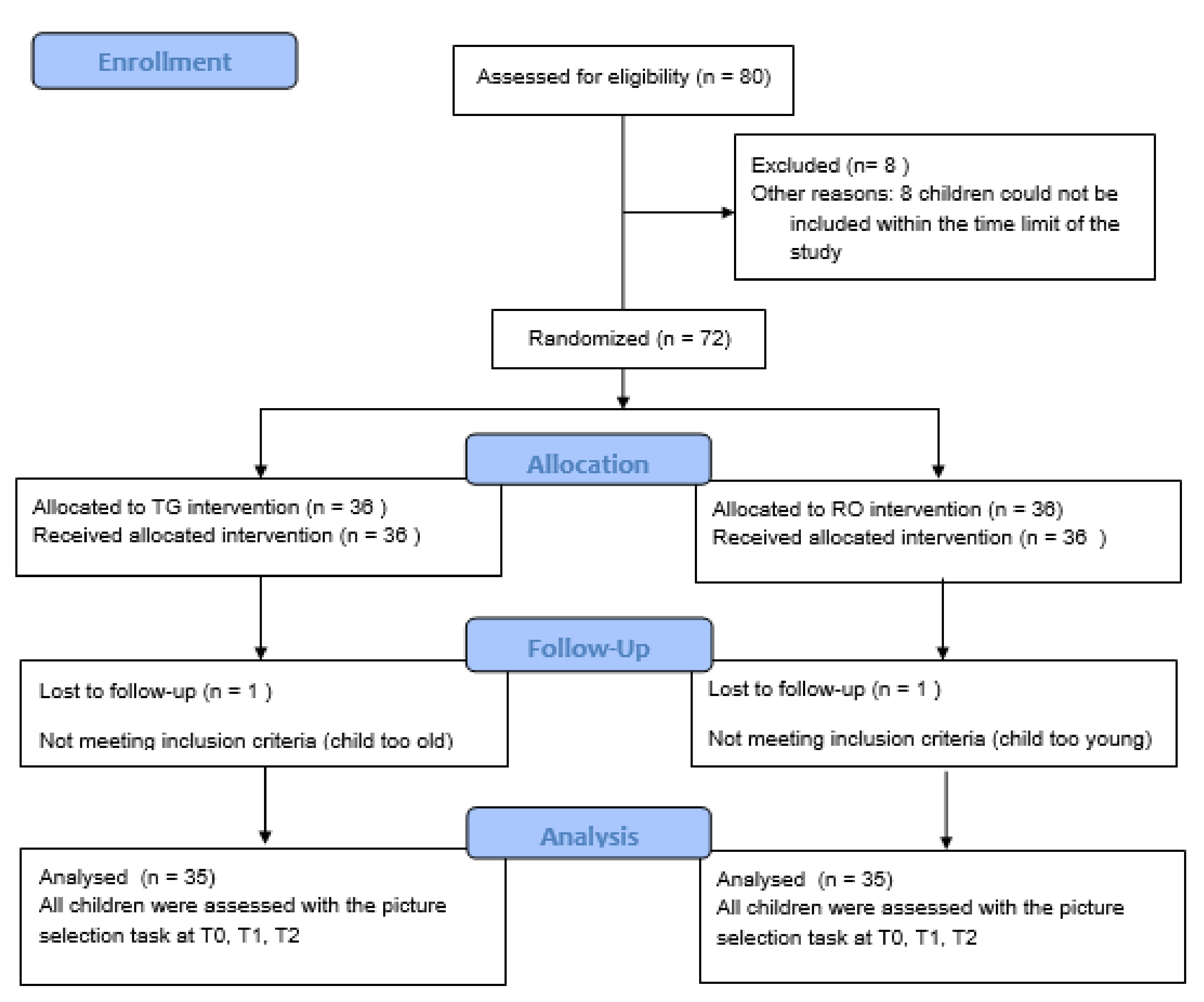
A randomized controlled non-inferiority trial [
16] was conducted comparing a novel vocabulary intervention using tablet games (TG) with standard intervention using real objects (RO) for 3-year-old children with DLD. All children visited special daycare groups for toddlers (2–5-year-old children) with DLD in the Netherlands. Both interventions consisted of 12 10-minute symbolic play sessions using 22 target words related to the theme of ‘kitchen ‘and ‘cooking’. The outcome was the number of new words learned by the child, measured with a one-out-of-four picture selection receptive vocabulary task. Receptive vocabulary was tested before the intervention started (T0), immediately following intervention (T1), and 5 weeks after intervention (T2). The children were randomly allocated to the two intervention conditions via stratified sampling (see
Figure 1 for the Consolidated Standards of Reporting Trials (CONSORT) diagram).
We planned to recruit 80 children with DLD, based on an a priori power analysis, but managed to enroll 72 children with DLD within the available time frame of the study.
2.1. Participants
The children for this study were recruited via 18 SLPs working in special daycare centers for young children with DLD in the Netherlands. In these centers, the children received multidisciplinary individual and group training from SLPs, pedagogical assistants, psychologists, social workers, and child physiotherapists. Groups usually consist of 8 children visiting the center 3–4 days a week. The inclusion criteria were an age range between 3;0 and 3;11 (years; months) and meeting the admission requirements for special daycare centers for young children with DLD in the Netherlands. These requirements entail scores on standardized language tests below 1.5 standard deviation, a non-verbal IQ score within the normal range (>70), no behavioral problems, no physical problems, no sensorineural hearing loss (>25 dB), and restricted communicative participation as judged by an SLP.
The assessment of the multilingual children was similar, with the exception that only standardized tests were used that had norms for multilingual children or trained interpreters were involved to evaluate assessing T1 of the children. All children already had received speech and language therapy in SLP practices prior to enrollment in the special day care centers.
A detailed description of the multidisciplinary language assessment procedures in the Netherlands can be found in [
17]. Each SLP selected 4 3-year-old children from their clinical caseload. Two children were eventually excluded from analysis because their birth dates turned out to be incorrect—one child was too young and another one too old—resulting in a total of 70 children, with 35 children in each intervention condition.
2.2. Intervention
The SLPs working at the daycare centers with the children delivered the intervention. Each SLP treated two children in the tablet condition and two in the real objects condition.
2.3. Procedure
Prior to the intervention phase, all 18 SLPs received 3 h of training on location at the special daycare centers. They were trained in delivering the vocabulary intervention using the tablet game as well as the real objects. Two SLPs were not able to attend these meetings; therefore, they received the training online via Skype. All SLPs had a tablet with the tablet game used in the intervention pre-installed. During the training, the following topics were addressed: the aim of the study and the study protocol, the test and intervention intervals, the target words chosen for the intervention (
Appendix A), and the scripts for the sessions to be used in both conditions (
Appendix B). Furthermore, they were instructed how to fill in and return the weekly logbooks and the importance of monitoring treatment fidelity this way. During the training, the SLPs practiced the intervention scripts in both the tablet game and real objects condition during role-play. Much emphasis was given to the prerequisite that the treatments in both conditions had to be as comparable as possible. Naturally, all SLPs are familiar with working with real objects during therapy. In addition, the best practices to deliver vocabulary therapy with tablet games were presented and practiced. The SLPs also received printed material containing the scripts, a list of target words, a roadmap for the treatment sessions, a logbook template, and a hand-out with tips and tricks on how to use tablet games during therapy. These tips and tricks were based on a study investigating the verbal and nonverbal strategies of SLPs working with tablet games in speech and language therapy. A key outcome of this study was that social interaction is crucial, and therefore, a key element of our intervention was that the child and therapist always played the game together [
18].
2.3.1. Word Lists and Scripts
The vocabulary intervention consisted of symbolic play sessions wherein the SLPs presented the 22 target words in a narrative, and the target words were also elicited via natural interaction and language facilitation strategies. The intervention was developed according to best evidence for word learning, supporting strategies such as interactive focused stimulation [
19] and frequent exposure to the target words in different narrative contexts [
14,
20,
21]. To control the content of the two intervention conditions, we developed vocabulary scripts for each session for use by the SLPs. These scripts were narratives with repetitions of the target words. The scripts were almost identical for both therapy conditions, but some sentences were adapted to fit either the tablet game or the play kitchen condition. All target words had to be presented at least once in each session. The target words in the scripts were all chosen from the theme ‘kitchen’ and were selected using several Dutch vocabulary lists for young children (see
Appendix A). We elaborate on this selection process in the section on the development of the vocabulary task below. The scripts consisted of several play activities and written sample sentences containing the target words. The SLPs could adapt the script to the language level of each individual child, as long as all target words were used, and all prescribed play activities were executed. They were instructed to (re)read the scripts prior to each intervention session so the target words could be presented fluently during the sessions and the SLPs could concentrate on the interaction.
2.3.2. Play Material: Play Kitchen and Tablet Game Kitchen
For the vocabulary intervention, the SLPs used a play kitchen with several kitchen requisites, such as a toaster, pots and pans, cutlery, and plastic food items. The tablet game was the entertainment game ‘My PlayHome’ (see
Figure 2) [
22]. This tablet game contained two kitchen scenes, which were used by the SLPs alternately. In cases where a daycare group did not have a play kitchen, it was provided by the research team. All SLPs downloaded the game on their tablets before the start of the intervention.
2.3.3. Intervention Delivery and Dosage
The intervention consisted of 12 10-min joint play sessions with the SLP and the individual child within an 8–9-week period. The sessions took place at the special daycare centers and were delivered by the child’s own SLP. Most SLPs treated four children, with two in each condition. However, four SLTs were employed part-time and worked in pairs at two of the daycare centers. Therefore, they participated in pairs, meaning that each of them treated the four children once a week, again with two children in each condition. These SLPs ensured that the weekly transitions between therapy sessions went smoothly during the intervention phase.
In each session, the SLPs used a script containing all 22 target words. During 11 sessions, the SLPs presented 2 of the 22 target words more frequently to the children (i.e., at least 5 times), while the other target words were presented only once. In this way, each target word would receive higher exposure during one of the sessions. In the last session, each target word was presented only once. In total, all target words were presented at least 16 times during the intervention period.
2.3.4. Treatment Fidelity
Treatment fidelity of the SLPs was checked by means of logbooks. After every session, the SLPs filled in a logbook reporting the session date, the target words that were presented once, and the two target words that were presented five times. In addition, they could write down comments for the researchers. These logbooks were sent to the researchers by email each week.
2.4. Outcomes
Outcome Measure
The outcome measure was the number of newly learned target words presented during the intervention, measured with a specially designed criterion-referenced one-out-of-four picture selection receptive vocabulary task. The task was administered before intervention started (T0), immediately following intervention (T1), and 5 weeks after intervention (T2). The task consisted of 22 target words from the theme kitchen and 22 control words. The ‘kitchen’ theme was chosen because it would fit the experience and vocabulary development of 3-year-old children with DLD. The control words were added to the vocabulary task because we wanted to control for incidental word learning. The control words came from the theme ‘house’ or ‘household’. The exposure to these words outside the therapy condition (at home) was regarded as comparable to words from the kitchen theme. The control words were not presented to the children during the intervention sessions.
The vocabulary task contained different word classes. Previous studies have suggested that out of 10 new words selected for vocabulary therapy, not only nouns, but at least 4 verbs or adverbs should be selected, because children with DLD appear to have more difficulties learning verbs than nouns [
23]. Following the Dutch handbook on therapy for children with DLD [
24], 60% nouns, 30% verbs, and 10% adverbs were selected as the target and control items for the vocabulary task. Several vocabulary lists were consulted to select appropriate words for our age group of children with DLD [
24,
25]. Words were selected that could be presented in both intervention conditions that suited the zone of proximal development for 3-year-old children with DLD and could be depicted as recognizable images in a picture selection task. In addition, some additional words were selected that were clearly presented in the tablet game and could also be presented in the real objects condition.
A consensus procedure within the research team, consisting of SLPs and clinical linguists, was used to select the test items. When consensus on an item could not be reached, the item was dropped, and another word was chosen. A list of the target and control words can be found in
Appendix A. Because the picture selection task had to be administered three times within a short time period, there was a possible learning effect. Therefore, three different versions of the vocabulary task were constructed. In each version, the items were presented in a different order, and the four pictures on each page were also scrambled. In total, the picture selection vocabulary test contained 44 items. Photographs were used to depict the words, and all images were controlled for size, sharpness, color, and overall uniformity. Each page contained a picture of a target or control word, accompanied by three distractors, either semantically related, phonologically related, or unrelated to the target or control word. Each version of the vocabulary task contained two practice items that were presented first. During the practice phase, extra instruction could be given to the children when necessary. The children were instructed to point at the picture that matched the word best.
The researchers that administered the picture selection tasks were blind to the intervention condition the children were assigned to during all three measurements (T0, T1, and T2). In general, the same researcher assessed the same group of children. In a few cases, when children were absent during assessment, an SLP from that special daycare center who was not involved in the study administered the task.
2.5. Sample Size
An a priori sample size was determined based on a power calculation in G*Power 3.1.9.2 [
26] for repeated measures ANOVA for within–between interaction with an effect size of 0.5, two groups, and three measurements, showing that a sample of 65 participants had a power of 95% to detect group differences (
p < 0.05). We chose a conservative effect size of 0.5. Marulis and Neuman [
27] concluded in a meta-analysis that young children’s language development benefitted from vocabulary intervention, with an overall effect size of 0.88. To be on the safe side, we decided to recruit 80 participants in the first phase of enrollment (see
Figure 1).
2.6. Randomization
In total, 72 children were enrolled in the study. The children were assigned to the TG or RO conditions using stratified sampling by author R.Z., who did not know the children and was not involved in the intervention. The enrolled children received care in 18 different daycare groups, and each child received the intervention from their own SLPs. Within each daycare group, four children were selected who were randomly assigned to the intervention conditions, leading to two children in each intervention condition per daycare group.
2.7. Blinding
Of course, blinding was not possible for the SLPs and the children participating in the intervention. However, the researchers administering the vocabulary task at T0, T1, and T2 were blinded and thus were unaware of the treatment conditions of the children.
2.8. Statistical Analysis
As we conducted a non-inferiority trial, we wanted to examine whether vocabulary therapy using tablets would yield similar results to a standard treatment using real objects. Our hypothesis was that we would not find statistically significant differences in vocabulary gains between the two intervention conditions or that this difference would not be clinically relevant (i.e., not larger than two words). At baseline T0, independent two-tailed t-tests were performed on the descriptives and vocabulary picture selection task scores of both intervention groups to check whether the groups were comparable. We used repeated measures ANOVA to analyze the group differences between the intervention condition, time measurement points (T0, T1, and T2), and between the target and control words. All data were analyzed with the IBM SPSS Statistics 25 software package. Assumptions of normality and sphericity were checked and were not violated.
3. Results
The data of 70 children with DLD (mean age: 3;6 years) were analyzed. The baseline characteristics of the participants are presented in
Table 1. The scores of the children for the standardized language tests and non-verbal IQ tests were drawn from the patient records of the children. These scores were not obtained at the start of the study but came from routine outcome monitoring performed regularly at the daycare groups. The standardized language test scores were between 0 and 12 months old, and most of these scores were less than 6 months old, while the non-verbal IQ scores were between 0 and 18 months old.
Independent two-tailed t-tests were used to analyze possible differences between the two intervention groups at baseline. The results show that the age in months did not differ between groups (
t(68) = −0.988,
p = 0.327). There were no group differences at baseline, making the two intervention groups comparable (receptive vocabulary scores (PPVT-NL)
t(58) = −1.223,
p = 0.226; Schlichting language comprehension scores
t(66) = −1.223,
p = 0.799; Schlichting word production scores
t(65) = 1.661,
p = 0.102; Schlichting sentence production scores
t(58) = 1.615,
p = 0.112; non-verbal IQ
t(58) = 0.242,
p = 0.810). In addition, independent two-tailed t-tests were performed at T0 on the vocabulary scores for the two conditions. There were no significant differences between the two conditions for either the target words (
t(68) = −1.543,
p = 0.128) or control words (
t(68) = −0.925,
p = 0.358). Lastly, a paired samples t-test at pre-test T0 yielded no significant difference between the target and control words (
t(69) = −1.383,
p = 0.171). The children obtained similar scores for both types of words.
Table 2 summarizes the group means and standard deviations for the number of correct target and control words on the receptive vocabulary task at the three time points.
According to the logbooks returned weekly by the SLPs, although all children received all treatment sessions, not all children received each treatment session as intended. For instance, occasionally two children were treated together in one session due to the absence of a child in a previous session. Another example is that the SLP sometimes presented the words that had to be presented five times in another order than established in the protocol. It could also be the case that not all target words were presented during a session because the child had poor attention during the session. These deviations from the protocol occurred in both intervention conditions, namely in 10 children in the TG condition and in 8 children in the RO condition.
To check for a possible influence of these deviations, statistical analyses were also performed with exclusion of the 18 children where the protocol was not followed strictly. First, the results of the statistical analyses of the total group of 70 children are presented. The children’s scores were analyzed with two (condition: tablet game vs. real objects) by two (type of words: target vs. control words) by three (time: T1 vs. T2 vs. T3) repeated measures analysis of variance (RM-ANOVA). There was no effect from the condition F(1, 68) = 0.553,
p = 0.460. There was only a significant effect for interaction between the time and type of word (F(2, 136) = 47.399,
p < 0.0005, partial η
2 = 0.606), meaning that the children learned more target words than control words.
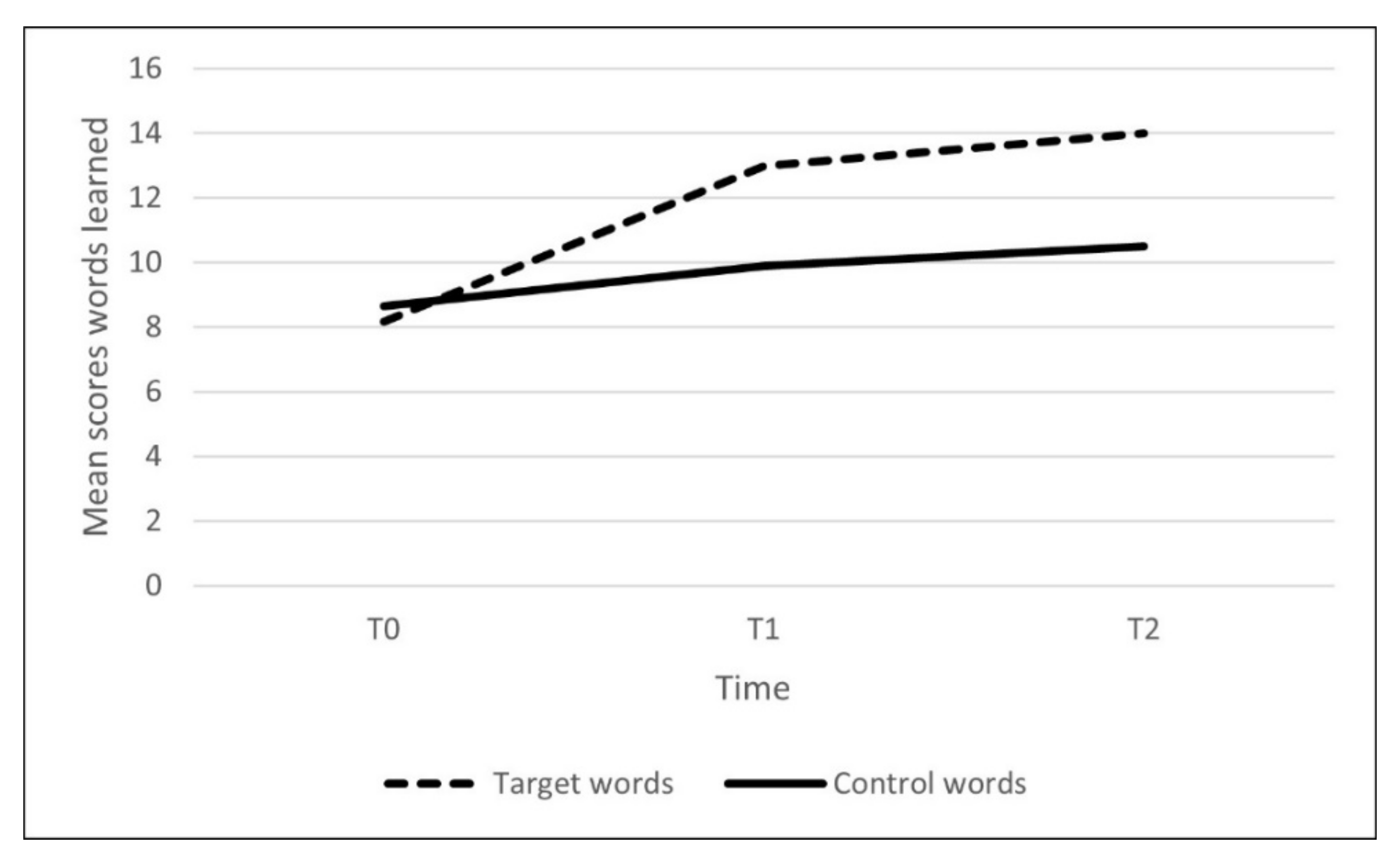
Figure 3 illustrates the number of new target and control words learned directly post-intervention and at the retention measurement, with a steeper curve in the target words compared with the control words. Partial η
2 effect sizes can be interpreted as follows: 0.01 = small effect, 0.06 = medium effect, and 0.14 = large effect.
Follow-up repeated measures ANOVA per type of word showed a growth of target words (F(2, 136) = 123.033, p < 0.0005, partial η² = 0.644). Post hoc tests showed that differences between T0 and T1 (p < 0.0005, partial η² = 0.690), T0 and T2 (p < 0.0005, partial η² = 0.746), and T1 and T2 (p = 0.032, partial η² = 0.092) were all statistically significant.
For the control words, the mean scores also differed significantly over time (F(2, 136) = 17.382, p < 0.0005). Post hoc tests yielded a significant difference between T0 and T1 (p < 0.0005, partial η² = 0.216) and T1 and T3 (p < 0.0005, partial η² = 0.300) but not between T1 and T2 (p = 0.221).
Because we wanted to know whether these results would change when the 18 children who did not receive all intervention sessions as intended were excluded (per-protocol analysis), the same analysis with the remaining 52 children was performed. Again, there was no effect from the condition F(1, 50) = 0.186, p = 0.668 and only a significant effect for the interaction between time and the type of word F(2, 49) = 35.379, p < 0.0005, partial η2 = 0.591, again meaning that the children learned more target words than control words. Because the results of this analysis with 52 children did not differ from the analysis with the total group of 70 children, the results of the total group of 70 participants were used.
4. Discussion
Our aim was to examine whether vocabulary intervention with tablet games was equally as effective as a standard intervention with traditional play material. Both in the total participant group of 70 children and in the smaller group of 52 children, who received the intervention exactly as protocolled, this was indeed the case. Three-year-old children with DLD learned as many new words in the tablet game condition as in the real objects condition. Our findings support the results from a prior study by Singer and Gerrits [
33], where only target words were used without the addition of control words to evaluate the influence of incidental word learning. In our study, more target words than control words were learned in both intervention conditions, meaning that the children learned more new words during intervention than could be accounted for by natural vocabulary growth. In a similar vein, when comparing traditional therapy with an interactive computer game, Wren and Roulstone [
34] found no difference in gains for phonological therapy between these two conditions.
In our study, contrary to other studies that tested the efficacy of computer tasks played individually by the child, the tablet game was played together with the SLP, who used similar prompting and language-stimulating techniques as in the symbolic play sessions with real objects. For our study, we developed a manual, ‘Playing tablet games together’, based on video analysis of therapy sessions with real objects and with games and a qualitative analysis of focus group discussions with SLPs [
18]. The latter analysis revealed that the most important difference between the study conditions was that more direction from the SLP and rules for turn-taking were needed when using tablet games. Otherwise, the children tended to hold the tablet and play the game on their own. This behavior is probably what they are used to doing in other settings, such as the home environment, where children play with their tablets independently. The SLPs mentioned that children liked to play the game together and discover the possibilities and hidden surprises.
With regard to the gains found in our study, our study shows that vocabulary intervention is effective. However, the magnitude of this effect was somewhat disappointing. On average, the children learned 6 new words (receptively) in 12 10-min sessions. Clearly, for many children with DLD, expanding their vocabulary is challenging. This result corroborates Rice et al. [
35], who found that preschool children with DLD were poorer at learning new words than children matched either by chronological age or by mean length of utterance (MLU). Although the children in our study were exposed to the target words multiple times during the intervention period, this apparently was not enough to acquire all the presented target words. It might be that the children needed more time to learn to match the target words to objects or concepts. The dosage of our 2 vocabulary interventions was 10 min in 12 sessions in 8–9 weeks (56–63 days). We chose this frequency and duration since it resembled the usual Dutch care and intensity of interventions mentioned in previous studies. A large survey across Europe revealed that the predominant frequency of therapy for children with DLD is 1 session a week for 30–45 min [
36]. A therapy session usually contains different activities addressing various aspects of language, such as vocabulary, communication, speech sound production, and sentence comprehension. Our choice of therapy intensity was also informed by the outcomes of the meta-analysis of Marulis and Neuman [
27] on the effects of vocabulary intervention on language development of preschool- and kindergarten-aged children. They summarized the broad ranges of dosage as follows: sessions longer than 20 min are not more effective than shorter ones, the median total number of sessions was 18, and the median duration was 42 days. Marulis and Neuman [
27] pointed out that vocabulary training targeted to a discrete set of skills (like in the present study, where we trained and evaluated a closed set of target words) might involve shorter-term intervention activities than those that are designed to enhance more global skills. More recently, Frizelle et al. [
21] reported a systematic review on the influence of dosage on the language outcomes of children with DLD. They could only include three studies looking at dosage and vocabulary training. Frizelle et al. concluded that research is in its infancy and there is too much variation between studies in dosage, dose, outcome, outcome measures, and age of children to inform clinical practices [
21].
Concerning our measurement task, Nash and Donaldson [
14] used five different tasks to evaluate word learning. On the basis of their comprehensive assessment, they suggested that children with DLD have difficulties with both the phonological and semantic aspects of word learning. Our study could not provide such insights, as we chose to use only receptive vocabulary as the outcome. We chose to measure passive word knowledge, assuming that this would be a relatively easy task, since matching words to objects or concepts is one of the first steps in word learning (e.g., [
37]). Furthermore, testing these young children with a word production task could have led to frustration when they would fail to name the pictures. In a picture-pointing task, a response can always be provided. Forced-choice, one-out-of-four picture selection tasks are frequently used to measure passive vocabulary in children (e.g., the standardized Peabody Picture Vocabulary Test, [
38]).
The follow-up results showed that at the end of the 5-week retention period, there was a significant growth in target words, although rather marginal, with a gain of approximately one extra word learned. No such gains were found for the control words, indicating that additional word learning did not take place for the untrained words. A positive point is that the newly learned words were still known at the follow-up.
Another point for discussion is that we first analyzed the whole group of 70 children and then performed a secondary analysis with the 52 children who, according to the logbooks from the SLPs, completed all sessions according to the protocol. This secondary analysis yielded the same results. This finding strengthens our results, because it can be argued that the outcome of our study is more ecologically valid and fitting common practice, where therapy delivery can be suboptimal, as these young children are not always fit, fully concentrated, or cooperative. We did not use a highly experimental design where children have to learn novel words or receive intervention in a highly controlled clinical setting. All children received multidisciplinary group and individual therapy in special care daycare groups for children with DLD from 2 to 5 years old, and this the trial was embedded in their individual speech and language therapy.
One might even argue that SLPs are unfamiliar with using tablet games as a relatively new medium, and hence the present results might be an underestimation of the real effect. For most of the children in our study, tablets were not a new medium; they were already familiar with tablets. Young children living in technology-based communities, such as the Netherlands, start using touch-screen tablets at an early age [
39]. Young children are used to tablets and, according to Geist [
40], tablets may impact the emergent literacy of preschoolers and also have the potential for oral language development. Although research on the effectiveness of using tablets in educational settings for young children is expanding, in the SLP domain, such research is still scarce. According to Zajc et al [
12], children with DLD prefer the tablet over table-top activities when treated by their SLPs, and their case study showed that tablets increased children’s motivation and time spent on exercises.
4.1. Limitations
A limitation of the study is the lack of robust and systematic fidelity measures. We used records (logbooks) evaluating the use of target words, scripts, and activities according to our protocol. Analysis of the records implies that intervention was administered as intended. In addition, we evaluated the delivery in phone calls with the participating SLPs. We did not systematically observe or record therapy sessions and therefore cannot be 100 percent sure that the SLPs followed the scripts or therapy protocol. However, since the only difference between the two interventions was the mode of delivery (i.e., tablet game or real objects), we expect that the risk of bias caused by non-fidelity was relatively small.
4.2. Implications for Practice
This study is of particular interest because we used an entertainment game for our intervention. Entertainment games are widely available and often relatively low-priced compared with educational or therapy games. For example, the price of the kitchen game we used was EUR 4.50 (USD 5.50). SLPs can use tablet games in similar ways to traditional play materials. Furthermore, they are often very creative in using play materials for a variety of different therapy goals, so entertainment games can be used for a wide range of therapy goals.
4.3. Future Directions
In this study, we only investigated the effect of tablet games on vocabulary intervention. It would be very interesting to investigate whether using tablet games is equally effective in therapy aimed at improving phonology, productive vocabulary, and morphosyntax.


 ,
, 
{kind=link}
{kind=link}
{kind=link}


