
Emotional Eating Interventions for Adults Living with Overweight or Obesity: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
- Whether interventions that address EE are effective for achieving weight loss and/or improving EE in adults living with overweight or obesity.
- Which psychological approach appears most effective for weight loss and/or improving EE for adults living with overweight or obesity.
2. Materials and Methods
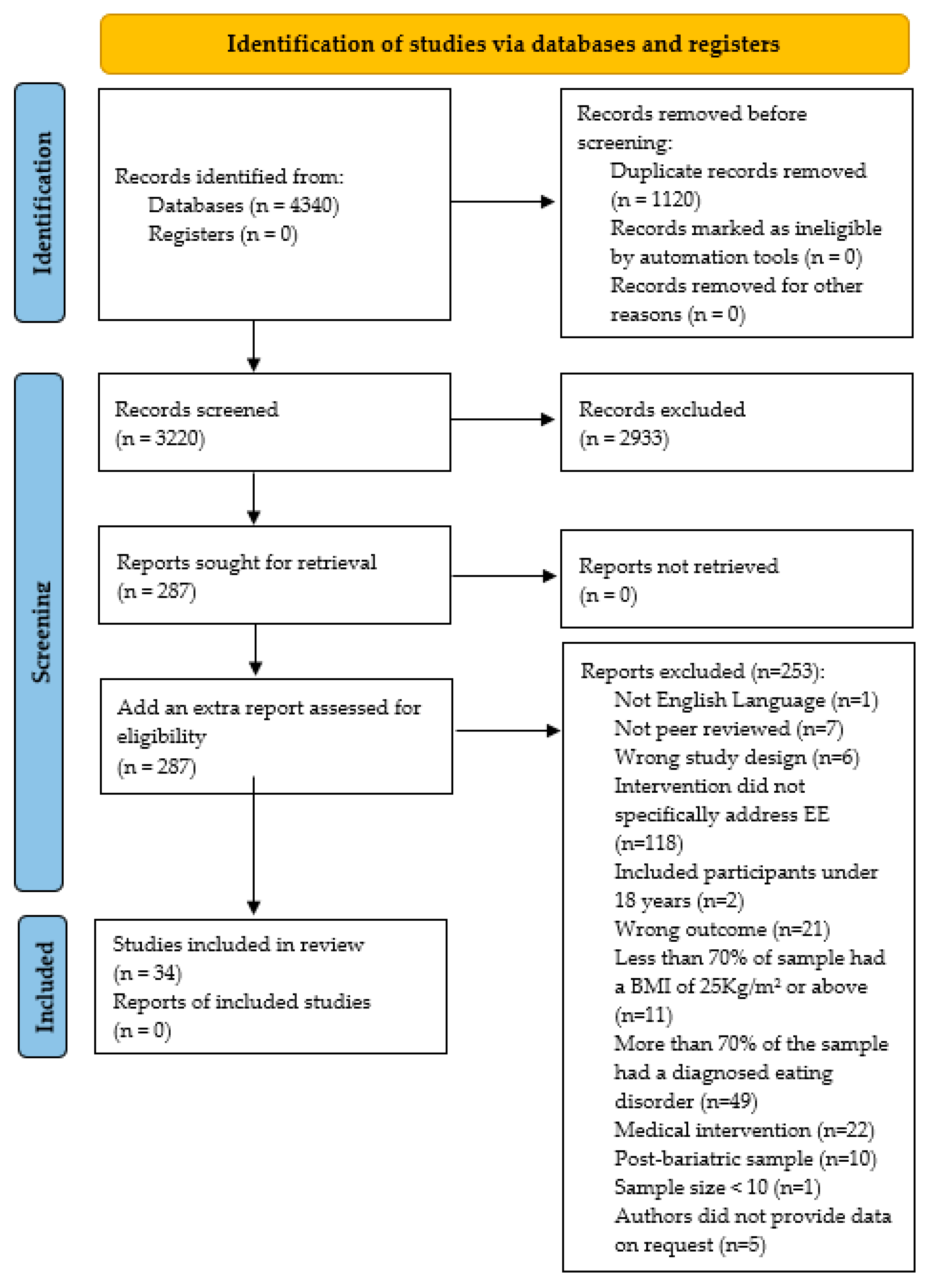
2.1. Eligibility Criteria, Search Strategy and Selection of Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Date, Intervention Name and Country | Study Characteristics | Intervention to Address EE | Outcomes Reported |
|---|---|---|---|
| Afari et al. (2019) [30] MOVE + ACT USA | Design: RCT Sample size: n = 88 (85 completers) Mean age: 57.3 years (SD: 9.9). Gender: 76.1% male, Ethnicity: 70.5% Caucasian, 17% African American, and 12% Hispanic | Interventions:
| Weight and EE |
| Annesi, et al. (2016) [31] LEARN USA | Design: Individually randomized group treatment trial Sample size: n = 103 Mean age: 47.8 years (SD: 7.9) Gender: 100% female Ethnicity: 84% White, 12% African American, and 4% other | Interventions:
| Weight and EE |
| Annesi (2019) [32] USA | Design: Individually randomized group treatment trial Sample size: n = 152 Mean age: 48.6 years (SD:7.0) Gender: 100% female Ethnicity: 80% White, 15% Black, 5% other | Interventions:
Group 1: 28 weeks, phone calls Group 2: 58 weeks, in person Group 3: 99 weeks, phone calls and in person | EE only |
| Bacon et al. (2005) [33] Health at Every Size USA | Design: Individually randomized group treatment trial Sample size: n = 35 completers at post-intervention. Mean age: HAES: 40.4 (SD:4.4); Diet: 41.4 years (SD:3.0) Gender: 100% female Ethnicity: Not reported | Interventions:
| Weight and EE |
| Carbine et al. (2021) [34] USA | Design: RCT Sample size: n = 100 Mean age: 28.05 years (SD:7.56) Gender: 53% Female Ethnicity: 81% Caucasian, 14% Hispanic, 5% other | Interventions:
| Weight and EE |
| Carpenter et al. (2019) [35] Mind Your Weight USA | Design: Individually randomized group treatment trial, pilot study Sample size: n = 75 Mean age: 47.3 years (SD:10.0) Gender: 92% Female Ethnicity: 65.3% White, 26.7% Black, 6.7% Hispanic, 1.3% Asian | Interventions:
| EE only |
| Chung et al. (2016) [36] USA | Design: Single group design, longitudinal study Sample size: n = 22 Mean age: 50.14 years (SD:9.0) Gender: 100% Female Ethnicity: 100% African American | Intervention:
| Weight and EE |
| Daubenmier et al. (2016) [37] SHINE USA | Design: RCT Sample size: n = 194 Mean age: 47.5 years (SD:12.7) Gender: 80% Female Ethnicity: 59.3% European, 12.9% African, 9.8% Asian/Pacific Islander, 11.9% Latina/Latino, 1% Native American, 5.1% other | Intervention:
| Weight only |
| Forman et al. (2013) [38] Mind your Health USA | Design: RCT Sample size: n = 128 (99 completers post-intervention) Mean age: 45.69 years (SD:12.81) Gender: Not reported Ethnicity: 62.3% Caucasian, 24.6% African American, 1.6% Asian, 3.8% Hispanic | Interventions:
| EE only |
| Frayn et al. (2020) [23] Switzerland | Design: Single group design Sample size: n = 32 Mean age: 46.71 years (SD:13.43) Gender: 87.5% Female, 12.5% Male Ethnicity: 78.1% Caucasian, 3.1% Middle Eastern, 3.1% Black, 3.1% Hispanic, 12.5% other | Intervention:
| EE only |
| Goldbacher et al. (2016) [24] USA | Design: Individually randomized group treatment trial Sample size: n = 79 Mean age: 45.6 years (SD:10.5) Gender: 95% Female, 5% Male Ethnicity: 80% African American, 11% White, 4% Hispanic, 5% other | Interventions:
| Weight and EE |
| Hanson et al. (2019) [39] UK | Design: Single group design Sample size: n = 53 (33 completers) Mean age: 44.4 years (SD:11.0) Gender: 78.8% Female Ethnicity: Not reported Mean weight: 126.3 kg (SD:36.1) | Intervention:
| Weight and EE |
| Hawkins et al. (2021) [40] POWER-UP USA | Design: Single group design Sample size: n = 48 Mean age: 43.58 years (SD:1.50) Gender: 85.4% Female Ethnicity: Not reported | Intervention:
| Weight and EE |
| Hepdurgun et al. (2020) [41] Turkey | Design: Individually randomized group treatment trial Sample size: n = 51 in the intervention group Mean age: 40.1 years (SD:9.96) Gender: 80.4% Female, 19.6% Male Ethnicity: Not reported | Intervention:
| Weight only |
| Hunot-Alexander et al. (2021) [42] UK | Design: Single group design with qualitative evaluation Sample size: n = 37 (weight data reported for 32) Mean age: 48.3 years (SD:10.9) Gender: 93.8% Female, 6.3% Male Ethnicity: 90.6% White, 9.4% non-White | Intervention:
| Weight only |
| Kearney et al. (2012) [43] USA | Design: Single group design Sample size: n = 48 (38 completers post-intervention) Mean age: 49 years (SD:10.7) Gender: 87.5% Male Ethnicity: 85.4% White, 4.2% Black, 6.3% Hispanic, 4.2% Asian/Pacific-Islander/Native American | Intervention:
| Weight and EE |
| Keränen et al. (2009) [44] LITE Finland | Design: Individually randomized group treatment trial Sample size: n = 20 completers in the intervention group Mean age: 52 years (SD: 7.0) Gender: 25% Male Ethnicity: Not reported | Intervention:
| Weight only |
| Kidd et al. (2013) [45] USA | Design: Single group design Sample size: n = 12 Mean age: 51.8 years (SD: 9.1)p Gender: 100% Female Ethnicity: 58.3% African American, 41.7% White | Intervention:
| Weight and EE |
| Kim et al. (2021) [46] Healthy Life Plan Korea | Design: RCT Sample size: n = 583 (369 completers post-intervention) Mean age: 53.68 years (SD:10.12) for the IG and 53.94 years (SD: 10.18) for the MG. Gender: 61.6% Female, 38.4% Male Ethnicity: Not reported | Intervention:
| EE only |
| Lillis et al. (2016) [47] USA | Design: RCT Sample size: n = 162 Mean age: 50.2 years (SD: 10.9) Gender: 85% Female, 15% Male Ethnicity: 5% Black/African American, 6% Hispanic, 1% Asian, 88% Caucasian | Intervention:
| Weight only and EE |
| Malkina-Pykh (2012) [48] Russia | Design: RCT Sample size: n = 104 (58 completers at post-intervention) Mean age: 37.6 years (SD:6.7) Gender: 69% Female, 31% Male Ethnicity: Not reported | Intervention:
| EE only |
| Manzoni et al. (2009) [49] Italy | Design: RCT Sample size: n = 40 in the two intervention groups Mean age: Not reported Gender: 100% Female Ethnicity: Not reported | Intervention:
| Weight only |
| Mason et al. (2018) [50] USA | Design: Single group design Sample size: n = 104 (61 completers at post-intervention) Mean age: 46.07 years (SD:14.64) Gender: Not reported Ethnicity: 68.3% White, 4.8% Black, 10.6% Hispanic/Latino, 9.6% Asian/Pacific Islander, 0.0% Native American, 1.0% declined to answer | Interventions:
| Weight and EE |
| Moraes et al. (2021) [51] Brazil | Design: RCT Sample size: n = 64 in the two intervention groups of interest Mean age: EH: 35.98 years (SD:6.76); IT + CBT: 36.18 years (SD:2.75) Gender: EH: 81.8% Female, 18.2% Male; IT +CBT: 77.4% Female, 22.6% Male Ethnicity: Not reported | Interventions:
| Weight and EE |
| Niemeier et al. (2012) [52] USA | Design: Single group design pilot Sample size: n = 21 (18 completers at post-intervention) Mean age: 52.2 years (SD:7.6) Gender: 90.5% Female, 9.5% Male Ethnicity: 90% non-Hispanic, 4.8% Hispanic, 4.8% other | Intervention:
| Weight and EE |
| Paans et al. (2020) [53] MooDFOOD Netherland | Design: RCT Sample size: n = 372 for intervention group Mean age: 47.8 years (SD:12.6) Gender: 78.2% Female Ethnicity: Not reported | Intervention:
| Weight and EE |
| Palmeira et al. (2017) [54] Kg-free Portugal | Design: RCT Sample size: n = 27 for intervention group Mean age: 41.97 years (SD: 8.79). Gender: 100% women Ethnicity: Not reported | Intervention:
| EE only |
| Rieger et al. (2017) [55] Australia | Design: RCT Sample size: n = 201 (118 completers post-intervention) Mean age: 47.01 years (SD:11.52) Gender: 73.6% Female | Intervention: Cognitive Behaviour Therapy (CBT):
| Weight and EE |
| Roosen et al. (2012) [21] Netherlands | Design: Pilot, single group design Sample size: n = 35 Mean age: 39.2 years (SD:11.02) Gender: 86% Female, 15% Male Ethnicity: Not reported | Intervention:
| EE only |
| Salvo et al. (2021) [56] MB-EAT Brazil | Design: Pilot, single group design, with mixed-methods evaluation Sample size: n = 20 Mean age: 48.15 years (SD:8.57) Gender: 100% Female Ethnicity: Not reported | Intervention:
| Weight only and EE |
| Sampaio et al. (2021) [57] Brazil | Design: RCT Sample size: n = 27 for intervention group Mean age: 49 years (SD:11.0) Gender: 100% Female Ethnicity: 7.4% White, 40.7% Black, 51.9% mixed | Intervention:
| EE only |
| Spadaro et al. (2017) [58] USA | Design: RCT Sample size: n = 46 Mean age: 45.2 years (SD:8.2) Gender: 87% Female, 13% Male Ethnicity: 78.3% Caucasian, 21.7% African American | Intervention:
| Weight and EE |
| Tham and Chong (2020) [59] Medical & Mind Weight Loss Redefine CBT Programme Australia | Design: Single group design Sample size: n = 120 Mean age: Not reported Gender: 57.5% Female, 42.5% Male | Intervention:
| Weight and EE |
| Thomas et al. (2019) [60] POWER and MORE POWER USA | Design: RCT Sample size: n = 51 Mean age: 57.92 years (SD: 10.04) Gender: 100% Female Ethnicity: 96% White, 2% Black/African American, 2% Hispanic/Latino | Intervention:
| Weight and EE |
2.2. Data Extraction
2.3. Critical Appraisal
2.4. Synthesis of Results and Analytical Strategy
3. Results
3.1. Study and Participant Characteristics
3.1.1. Study Characteristics
3.1.2. Participant Characteristics
3.2. Variables and Measurement Tools
3.2.1. Weight and BMI
3.2.2. Emotional Eating
3.3. Interventions
3.3.1. Behavioural Weight Loss
3.3.2. Mindfulness
3.3.3. Acceptance-Based Interventions
3.3.4. Combined Interventions
3.3.5. Behavioural Therapy
3.3.6. Cognitive Behavioural Therapy
3.3.7. Dialectical Behavioural Therapy
3.3.8. Other Therapies
3.4. Meta-Analysis
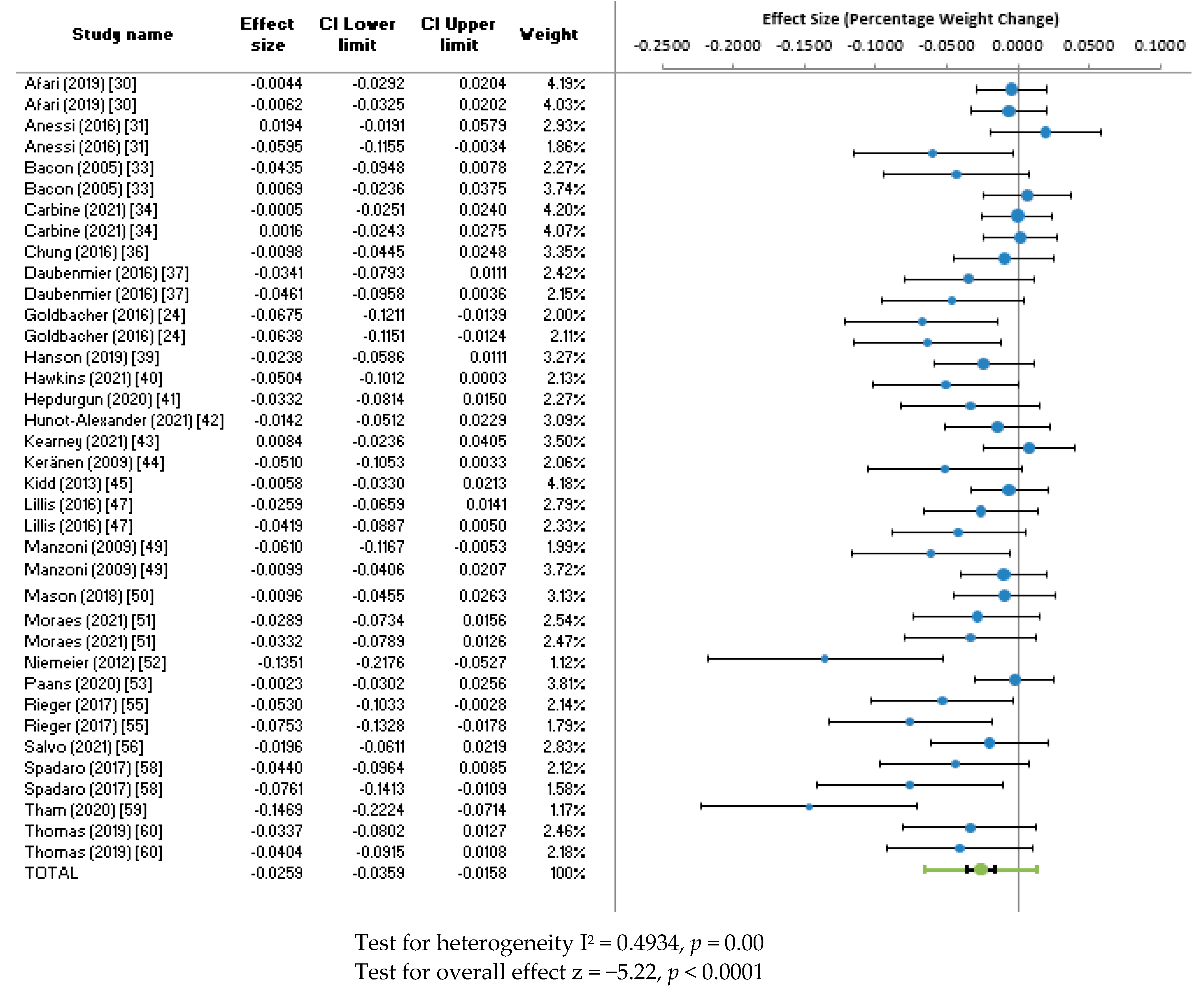
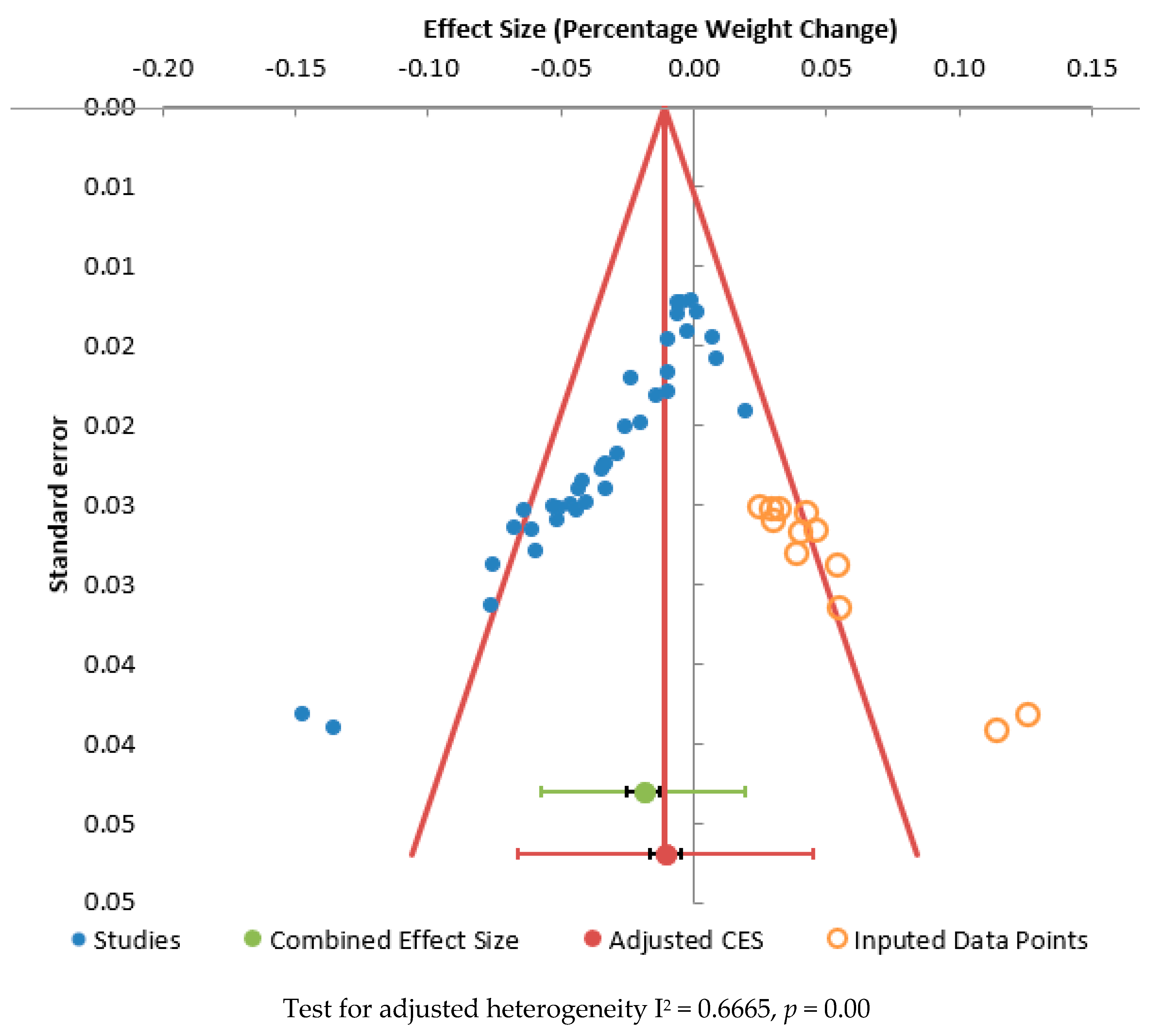
3.4.1. Weight
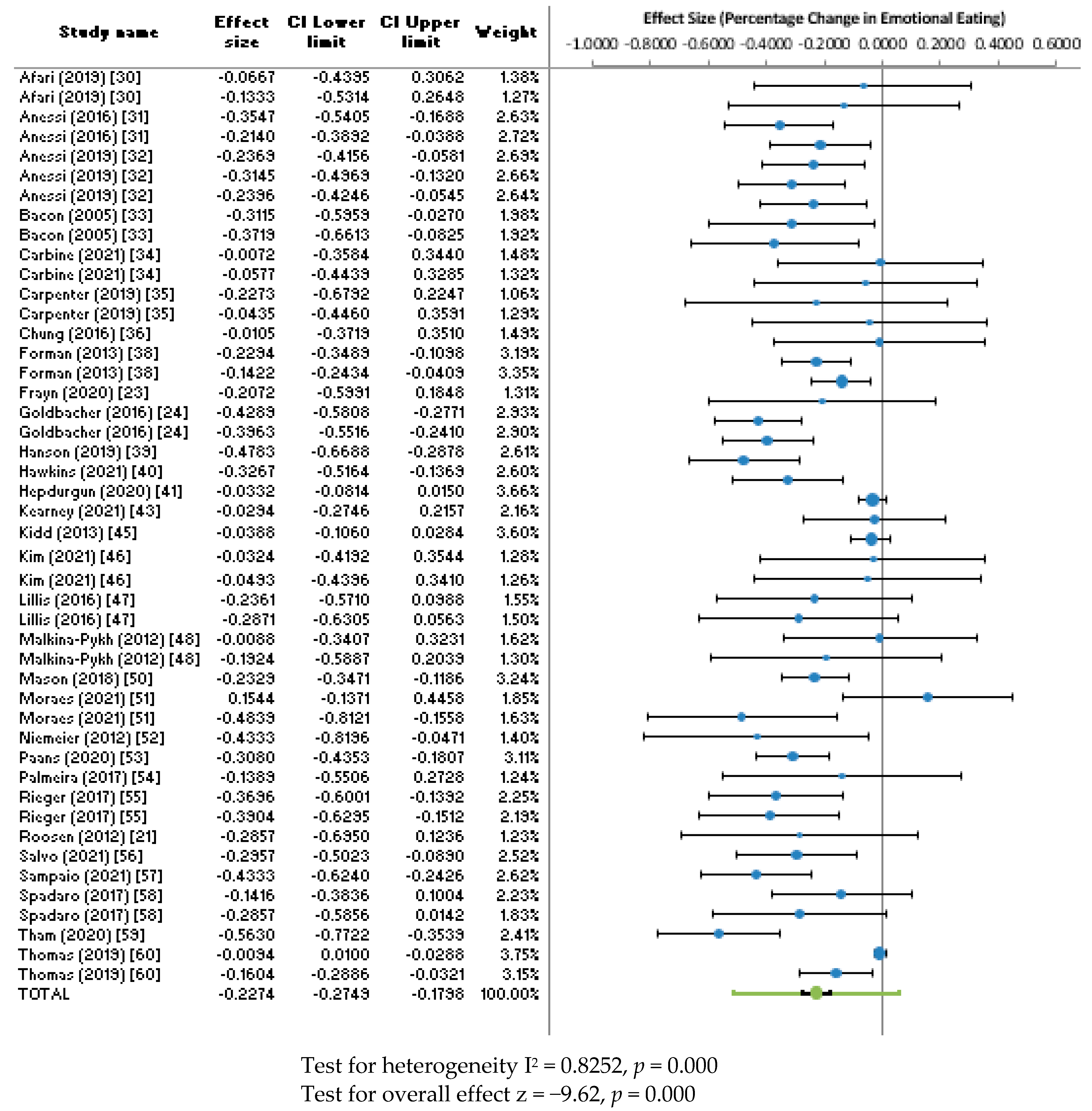
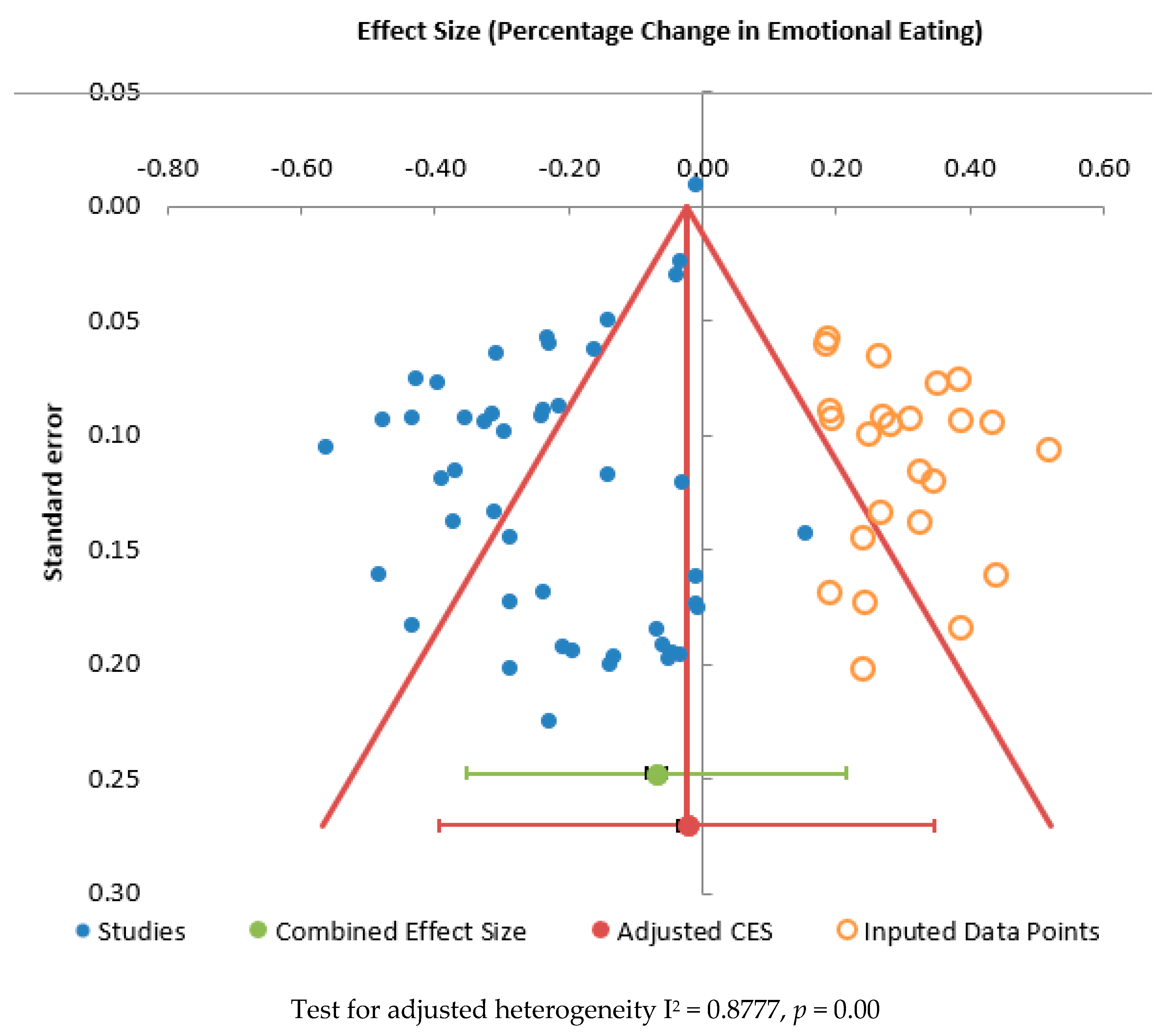
3.4.2. Emotional Eating Score
3.5. Methodological Quality
4. Discussion
4.1. Intervention Effects on Weight
4.2. Interventions for Improving Emotional Eating
4.3. Intervention Setting and Mode of Delivery
4.4. Screening Tools for Emotional Eating
4.5. Demographic Differences
4.6. Strengths and Limitations
4.6.1. Strengths
4.6.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- NHS Digital Statistics on Obesity, Physical Activity and Diet, England. 2020. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-obesity-physical-activity-and-diet/england-2020/part-3-adult-obesity-copy (accessed on 15 June 2022).
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 30 January 2022).
- National Institute for Health and Care Excellence (NICE). Obesity: Identification, Assessment and Management. Clinical Guideline [CG189]. Available online: https://www.nice.org.uk/guidance/cg189/ifp/chapter/obesity-and-being-overweight (accessed on 31 January 2022).
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J. Am. Coll. Cardiol. 2014, 63, 2985–3023. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Butryn, M.L. Behavioral treatment of obesity. Endocrinol. Metab. Clin. N. Am. 2003, 32, 981–1003. [Google Scholar] [CrossRef] [PubMed]
- Gudzune, K.A.; Doshi, R.S.; Mehta, A.K.; Chaudhry, Z.W.; Jacobs, D.K.; Vakil, R.M.; Lee, C.J.; Bleich, S.N.; Clark, J.M. Efficacy of commercial weight-loss programs: An updated systematic review. Ann. Intern. Med. 2015, 162, 501–512. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.S.; Woo, J. Prevention of overweight and obesity: How effective is the current public health approach. Int. J. Environ. Res. Public Health 2010, 7, 765–783. [Google Scholar] [CrossRef] [PubMed]
- Brownell, K.D.; Wadden, T.A. The Heterogeneity of Obesity: Fitting Treatments to Individuals—Republished Article. Behav. Ther. 2016, 47, 950–965. [Google Scholar] [CrossRef] [PubMed]
- Limbers, C.A.; Summers, E. Emotional eating and weight status in adolescents: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 991. [Google Scholar] [CrossRef] [PubMed]
- Gibson, E.L. The psychobiology of comfort eating: Implications for neuropharmacological interventions. Behav. Pharmacol. 2012, 23, 442–460. [Google Scholar] [CrossRef]
- Konttinen, H. Emotional eating and obesity in adults: The role of depression, sleep and genes. Proc. Nutr. Soc. 2020, 79, 283–289. [Google Scholar] [CrossRef]
- Van Strien, T. Causes of Emotional Eating and Matched Treatment of Obesity. Curr. Diabetes Rep. 2018, 18, 35. [Google Scholar] [CrossRef]
- Fuente González, C.E.; Chávez-Servín, J.L.; de la Torre-Carbot, K.; Ronquillo González, D.; Aguilera Barreiro, M.d.l.Á.; Ojeda Navarro, L.R. Relationship between Emotional Eating, Consumption of Hyperpalatable Energy-Dense Foods, and Indicators of Nutritional Status: A Systematic Review. J. Obes. 2022, 2022, 4243868. [Google Scholar] [CrossRef]
- Reichenberger, J.; Schnepper, R.; Arend, A.K.; Blechert, J. Emotional eating in healthy individuals and patients with an eating disorder: Evidence from psychometric, experimental and naturalistic studies. Proc. Nutr. Soc. 2020, 79, 290–299. [Google Scholar] [CrossRef] [PubMed]
- Macht, M. How emotions affect eating: A five-way model. Appetite 2008, 50, 1–11. [Google Scholar] [CrossRef]
- Greeno, C.G.; Wing, R.R. Stress-induced eating. Psychol. Bull. 1994, 115, 444–464. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (5th Edition, Text Review), 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2022. [Google Scholar] [CrossRef]
- Eichen, D.M.; Chen, E.; Boutelle, K.N.; McCloskey, M.S. Behavioral evidence of emotion dysregulation in binge eaters. Appetite 2017, 111, 1–6. [Google Scholar] [CrossRef]
- Nguyen-Rodriguez, S.T.; Unger, J.B.; Spruijt-Metz, D. Psychological determinants of emotional eating in adolescence. Eat. Disord. 2009, 17, 211–224. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.J.; Silva, M.N.; Coutinho, S.R.; Palmeira, A.L.; Mata, J.; Vieira, P.N.; Carraça, E.V.; Santos, T.C.; Sardinha, L.B. Mediators of weight loss and weight loss maintenance in middle-aged women. Obesity 2010, 18, 725–735. [Google Scholar] [CrossRef]
- Roosen, M.A.; Safer, D.; Adler, S.; Cebolla, A.; van Strien, T. Group dialectical behavior therapy adapted for obese emotional eaters: A pilot study. Nutr. Hosp. 2012, 27, 1141–1147. [Google Scholar] [CrossRef]
- Van de Laar, F.A.; van de Lisdonk, E.H.; Lucassen, P.L.; Stafleu, A.; Mulder, J.; van den Hoogen, H.J.; Rutten, G.E.; van Weel, C. Eating behaviour and adherence to diet in patients with Type 2 diabetes mellitus. Diabet. Med. 2006, 23, 788–794. [Google Scholar] [CrossRef]
- Frayn, M.; Khanyari, S.; Knäuper, B. A 1-day acceptance and commitment therapy workshop leads to reductions in emotional eating in adults. Eat. Weight. Disord. 2020, 25, 1399–1411. [Google Scholar] [CrossRef]
- Goldbacher, E.; La Grotte, C.; Komaroff, E.; Vander Veur, S.; Foster, G.D. An initial evaluation of a weight loss intervention for individuals who engage in emotional eating. J. Behav. Med. 2016, 39, 139–150. [Google Scholar] [CrossRef]
- Chew, H.S.J.; Lau, S.T.; Lau, Y. Weight-loss interventions for improving emotional eating among adults with high body mass index: A systematic review with meta-analysis and meta-regression. Eur. Eat. Disord. Rev. 2022, 30, 304–327. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Conn, V.S.; Coon Sells, T.G. WJNR welcomes umbrella reviews. West. J. Nurs. Res. 2014, 36, 147–151. [Google Scholar] [CrossRef]
- Horsley, T.; Dingwall, O.; Sampson, M. Checking reference lists to find additional studies for systematic reviews. Cochrane Database Syst. Rev. 2011, 2011, Mr000026. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Afari, N.; Herbert, M.S.; Godfrey, K.M.; Cuneo, J.G.; Salamat, J.S.; Mostoufi, S.; Gasperi, M.; Ober, K.; Backhaus, A.; Rutledge, T.; et al. Acceptance and commitment therapy as an adjunct to the MOVE! programme: A randomized controlled trial. Obes. Sci. Pract. 2019, 5, 397–407. [Google Scholar] [CrossRef]
- Annesi, J.J.; Mareno, N.; McEwen, K. Psychosocial predictors of emotional eating and their weight-loss treatment-induced changes in women with obesity. Eat. Weight. Disord. 2016, 21, 289–295. [Google Scholar] [CrossRef]
- Annesi, J.J. Relationship of Emotional Eating and Mood Changes Through Self-Regulation Within Three Behavioral Treatments for Obesity. Psychol. Rep. 2019, 122, 1689–1706. [Google Scholar] [CrossRef] [PubMed]
- Bacon, L.; Stern, J.S.; Van Loan, M.D.; Keim, N.L. Size acceptance and intuitive eating improve health for obese, female chronic dieters. J. Am. Diet. Assoc. 2005, 105, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Carbine, K.A.; Muir, A.M.; Allen, W.D.; LeCheminant, J.D.; Baldwin, S.A.; Jensen, C.D.; Kirwan, C.B.; Larson, M.J. Does inhibitory control training reduce weight and caloric intake in adults with overweight and obesity? A pre-registered, randomized controlled event-related potential (ERP) study. Behav. Res. Ther. 2021, 136, 103784. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, K.M.; Vickerman, K.A.; Salmon, E.E.; Javitz, H.S.; Epel, E.S.; Lovejoy, J.C. A Randomized Pilot Study of a Phone-Based Mindfulness and Weight Loss Program. Behav. Med. 2019, 45, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.; Zhu, S.; Friedmann, E.; Kelleher, C.; Kozlovsky, A.; Macfarlane, K.W.; Tkaczuk, K.H.; Ryan, A.S.; Griffith, K.A. Weight loss with mindful eating in African American women following treatment for breast cancer: A longitudinal study. Support. Care Cancer 2016, 24, 1875–1881. [Google Scholar] [CrossRef]
- Daubenmier, J.; Moran, P.J.; Kristeller, J.; Acree, M.; Bacchetti, P.; Kemeny, M.E.; Dallman, M.; Lustig, R.H.; Grunfeld, C.; Nixon, D.F.; et al. Effects of a mindfulness-based weight loss intervention in adults with obesity: A randomized clinical trial. Obesity 2016, 24, 794–804. [Google Scholar] [CrossRef]
- Forman, E.M.; Butryn, M.L.; Juarascio, A.S.; Bradley, L.E.; Lowe, M.R.; Herbert, J.D.; Shaw, J.A. The mind your health project: A randomized controlled trial of an innovative behavioral treatment for obesity. Obesity 2013, 21, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Hanson, P.; Shuttlewood, E.; Halder, L.; Shah, N.; Lam, F.T.; Menon, V.; Barber, T.M. Application of Mindfulness in a Tier 3 Obesity Service Improves Eating Behavior and Facilitates Successful Weight Loss. J. Clin. Endocrinol. Metab. 2019, 104, 793–800. [Google Scholar] [CrossRef]
- Hawkins, M.A.W.; Colaizzi, J.M.; Cole, A.B.; Keirns, N.G.; Smith, C.E.; Stout, M.; Chaney, J.; Sawhney, M.; Gahn, D. Pilot trial of acceptance-based behavioral weight loss and neurocognition among American Indians. Behav. Ther. 2021, 52, 350–364. [Google Scholar] [CrossRef] [PubMed]
- Hepdurgun, C.; Özalay, Ö.; Pırıldar, Ş.; Rudarlı Nalçakan, G.; Saygılı, L.F.; Seçkiner, S.; Ünalır, M.O.; Elbi, H. Testing an Internet-Based Turkish Obesity Behavioral Therapy Program: A Randomized Study. Turk Psikiyatr. Derg. 2020, 31, 41–47. [Google Scholar] [CrossRef]
- Hunot-Alexander, C.H.; Fildes, A.; Johnson, F.; Beeken, R.J. Brief ‘Appetitive Trait Tailored Intervention’: Development in a sample of adults with overweight and obesity. Behav. Chang. 2022, 39, 106–122. [Google Scholar] [CrossRef]
- Kearney, D.J.; Milton, M.L.; Malte, C.A.; McDermott, K.A.; Martinez, M.; Simpson, T.L. Participation in mindfulness-based stress reduction is not associated with reductions in emotional eating or uncontrolled eating. Nutr. Res. 2012, 32, 413–420. [Google Scholar] [CrossRef]
- Keränen, A.M.; Savolainen, M.J.; Reponen, A.H.; Kujari, M.L.; Lindeman, S.M.; Bloigu, R.S.; Laitinen, J.H. The effect of eating behavior on weight loss and maintenance during a lifestyle intervention. Prev. Med. 2009, 49, 32–38. [Google Scholar] [CrossRef]
- Kidd, L.I.; Graor, C.H.; Murrock, C.J. A mindful eating group intervention for obese women: A mixed methods feasibility study. Arch. Psychiatr. Nurs. 2013, 27, 211–218. [Google Scholar] [CrossRef]
- Kim, S.K.; Rodriguez Rocha, N.P.; Kim, H. Eating control and eating behavior modification to reduce abdominal obesity: A 12-month randomized controlled trial. Nutr. Res. Pract. 2021, 15, 38–53. [Google Scholar] [CrossRef]
- Lillis, J.; Niemeier, H.M.; Thomas, J.G.; Unick, J.; Ross, K.M.; Leahey, T.M.; Kendra, K.E.; Dorfman, L.; Wing, R.R. A randomized trial of an acceptance-based behavioral intervention for weight loss in people with high internal disinhibition. Obesity 2016, 24, 2509–2514. [Google Scholar] [CrossRef]
- Malkina-Pykh, I.G. Effectiveness of rhythmic movement therapy for disordered eating behaviors and obesity. Span. J. Psychol. 2012, 15, 1371–1387. [Google Scholar] [CrossRef]
- Manzoni, G.M.; Pagnini, F.; Gorini, A.; Preziosa, A.; Castelnuovo, G.; Molinari, E.; Riva, G. Can relaxation training reduce emotional eating in women with obesity? An exploratory study with 3 months of follow-up. J. Am. Diet. Assoc. 2009, 109, 1427–1432. [Google Scholar] [CrossRef] [PubMed]
- Mason, A.E.; Jhaveri, K.; Cohn, M.; Brewer, J.A. Testing a mobile mindful eating intervention targeting craving-related eating: Feasibility and proof of concept. J. Behav. Med. 2018, 41, 160–173. [Google Scholar] [CrossRef] [PubMed]
- Moraes, A.d.S.; Padovani, R.d.C.; La Scala Teixeira, C.V.; Cuesta, M.G.S.; Gil, S.d.S.; de Paula, B.; dos Santos, G.M.; Gonçalves, R.T.; Dâmaso, A.R.; Oyama, L.M.; et al. Cognitive Behavioral Approach to Treat Obesity: A Randomized Clinical Trial. Front. Nutr. 2021, 8, 611217. [Google Scholar] [CrossRef] [PubMed]
- Niemeier, H.M.; Leahey, T.; Palm Reed, K.; Brown, R.A.; Wing, R.R. An acceptance-based behavioral intervention for weight loss: A pilot study. Behav. Ther. 2012, 43, 427–435. [Google Scholar] [CrossRef]
- Paans, N.P.G.; Bot, M.; Brouwer, I.A.; Visser, M.; Gili, M.; Roca, M.; Hegerl, U.; Kohls, E.; Owens, M.; Watkins, E.; et al. Effects of food-related behavioral activation therapy on eating styles, diet quality and body weight change: Results from the MooDFOOD Randomized Clinical Trial. J. Psychosom. Res. 2020, 137, 110206. [Google Scholar] [CrossRef]
- Palmeira, L.; Pinto-Gouveia, J.; Cunha, M. Exploring the efficacy of an acceptance, mindfulness & compassionate-based group intervention for women struggling with their weight (Kg-Free): A randomized controlled trial. Appetite 2017, 112, 107–116. [Google Scholar] [CrossRef]
- Rieger, E.; Treasure, J.; Murray, K.; Caterson, I. The use of support people to improve the weight-related and psychological outcomes of adults with obesity: A randomised controlled trial. Behav. Res. Ther. 2017, 94, 48–59. [Google Scholar] [CrossRef]
- Salvo, V.; Sanudo, A.; Kristeller, J.; Schveitzer, M.C.; Martins, P.; Favarato, M.L.; Demarzo, M. Mindful eating for overweight and obese women in Brazil: An exploratory mixed-methods pilot study. Nutr. Health 2021, 28, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, C.V.S.; Magnavita, G.; Ladeia, A.M. Effect of Healing Meditation on stress and eating behavior in overweight and obese women: A randomized clinical trial. Complement. Ther. Clin. Pract. 2021, 45, 101468. [Google Scholar] [CrossRef] [PubMed]
- Spadaro, K.C.; Davis, K.K.; Sereika, S.M.; Gibbs, B.B.; Jakicic, J.M.; Cohen, S.M. Effect of mindfulness meditation on short-term weight loss and eating behaviors in overweight and obese adults: A randomized controlled trial. J. Complement. Integr. Med. 2017, 15, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Tham, M.; Chong, T.W. Evaluation of an online cognitive behavioural therapy weight loss programme as an adjunct to anti-obesity medications and lifestyle interventions. Australas Psychiatry 2020, 28, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.A.; Mijangos, J.L.; Hansen, P.A.; White, S.; Walker, D.; Reimers, C.; Beck, A.C.; Garland, E.L. Mindfulness-Oriented Recovery Enhancement Restructures Reward Processing and Promotes Interoceptive Awareness in Overweight Cancer Survivors: Mechanistic Results From a Stage 1 Randomized Controlled Trial. Integr. Cancer Ther. 2019, 18, 1534735419855138. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP (Randomised Controlled Trial Checklist). Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 15 June 2022).
- JBI. Checklist for Quasi-Experimental Studies (Non-Randomised Experimental Studies). Available online: https://jbi.global/critical-appraisal-tools (accessed on 8 January 2022).
- Okorodudu, D.O.; Jumean, M.F.; Montori, V.M.; Romero-Corral, A.; Somers, V.K.; Erwin, P.J.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Braden, O.B.W. Pilot study of a treatment using dialectical behavioral therapy skills for adults with overweight/obesity and emotional eating. J. Contemp. Psychother. 2021, 51, 21–29. [Google Scholar] [CrossRef]
- Suurmond, R.; van Rhee, H.; Hak, T. Introduction, comparison, and validation of Meta-Essentials: A free and simple tool for meta-analysis. Res. Synth. Methods 2017, 8, 537–553. [Google Scholar] [CrossRef] [Green Version]
- Van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Arnow, B.; Kenardy, J.; Agras, W.S. The Emotional Eating Scale: The development of a measure to assess coping with negative affect by eating. Int. J. Eat. Disord. 1995, 18, 79–90. [Google Scholar] [CrossRef]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Messick, S. The Eating Inventory; Psychological Corporation: San Antonio, TX, USA, 1988. [Google Scholar]
- Framson, C.; Kristal, A.R.; Schenk, J.M.; Littman, A.J.; Zeliadt, S.; Benitez, D. Development and validation of the mindful eating questionnaire. J. Am. Diet. Assoc. 2009, 109, 1439–1444. [Google Scholar] [CrossRef]
- Cotter, E.W.; Kelly, N.R. Binge Eating Scale (BES). In Encyclopedia of Feeding and Eating Disorders; Wade, T., Ed.; Springer: Singapore, 2016; pp. 1–5. [Google Scholar]
- Garaulet, M.; Canteras, M.; Morales, E.; López-Guimera, G.; Sánchez-Carracedo, D.; Corbalán-Tutau, M.D. Validation of a questionnaire on emotional eating for use in cases of obesity: The Emotional Eater Questionnaire (EEQ). Nutr. Hosp. 2012, 27, 645–651. [Google Scholar] [CrossRef]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The eating attitudes test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef]
- Masheb, R.M.; Grilo, C.M. Emotional overeating and its associations with eating disorder psychopathology among overweight patients with binge eating disorder. Int. J. Eat. Disord. 2006, 39, 141–146. [Google Scholar] [CrossRef]
- Kesten, D.; Scherwitz, L. Whole-person Integrative Eating: A Program for Treating Overeating, Overweight, and Obesity. Integr. Med. 2015, 14, 42–50. [Google Scholar]
- Meule, A.; Hermann, T.; Kübler, A. A short version of the Food Cravings Questionnaire-Trait: The FCQ-T-reduced. Front. Psychol. 2014, 5, 190. [Google Scholar] [CrossRef] [PubMed]
- Poelman, M.P.; de Vet, E.; Velema, E.; Seidell, J.C.; Steenhuis, I.H. Behavioural strategies to control the amount of food selected and consumed. Appetite 2014, 72, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Kristeller, J.; Wolever, R.Q.; Sheets, V. Mindfulness-Based Eating Awareness Training (MB-EAT) for Binge Eating: A Randomized Clinical Trial. Mindfulness 2014, 5, 282–297. [Google Scholar] [CrossRef]
- Hamilton, J.; Fawson, S.; May, J.; Andrade, J.; Kavanagh, D.J. Brief guided imagery and body scanning interventions reduce food cravings. Appetite 2013, 71, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Forman, E.M.; Butryn, M.L. A new look at the science of weight control: How acceptance and commitment strategies can address the challenge of self-regulation. Appetite 2015, 84, 171–180. [Google Scholar] [CrossRef]
- Giusti, E.M.; Spatola, C.A.; Brunani, A.; Kumbhare, D.; Oral, A.; Ilieva, E.; Kiekens, C.; Pietrabissa, G.; Manzoni, G.M.; Imamura, M.; et al. ISPRM/ESPRM guidelines on Physical and Rehabilitation Medicine professional practice for adults with obesity and related comorbidities. Eur. J. Phys. Rehabil. Med. 2020, 56, 496–507. [Google Scholar] [CrossRef] [PubMed]
- Safer, D.L.; Telch, C.F.; Chen, E.Y. Dialectical Behavior Therapy for Binge Eating and Bulimia; Guilford Press: New York, NY, USA, 2009. [Google Scholar]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Frayn, M.; Knäuper, B. Emotional Eating and Weight in Adults: A Review. Curr. Psychol. 2018, 37, 924–933. [Google Scholar] [CrossRef]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- Carroll, E.A.; Czerwinski, M.; Roseway, A.; Kapoor, A.; Johns, P.; Rowan, K.; Schraefel, M. Food and mood: Just-in-time support for emotional eating. In Proceedings of the 2013 Humaine Association Conference on Affective Computing and Intelligent Interaction, Geneva, Switzerland, 2–5 September 2013; pp. 252–257. [Google Scholar]
- Otte, C. Cognitive behavioral therapy in anxiety disorders: Current state of the evidence. Dialogues Clin. Neurosci. 2011, 13, 413–421. [Google Scholar] [CrossRef]
- Guastella, A.J.; Dadds, M.R. Cognitive-behavioural emotion writing tasks: A controlled trial of multiple processes. J. Behav. Ther. Exp. Psychiatry 2008, 39, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Glisenti, K.; Strodl, E. Cognitive Behavior Therapy and Dialectical Behavior Therapy for Treating Obese Emotional Eaters. Clin. Case Stud. 2012, 11, 71–88. [Google Scholar] [CrossRef]
- Forman, E.M.; Hoffman, K.L.; Juarascio, A.S.; Butryn, M.L.; Herbert, J.D. Comparison of acceptance-based and standard cognitive-based coping strategies for craving sweets in overweight and obese women. Eat. Behav. 2013, 14, 64–68. [Google Scholar] [CrossRef]
- Järvelä-Reijonen, E.; Karhunen, L.; Sairanen, E.; Muotka, J.; Lindroos, S.; Laitinen, J.; Puttonen, S.; Peuhkuri, K.; Hallikainen, M.; Pihlajamäki, J.; et al. The effects of acceptance and commitment therapy on eating behavior and diet delivered through face-to-face contact and a mobile app: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 22. [Google Scholar] [CrossRef]
- Gaesser, G.A.; Angadi, S.S.; Sawyer, B.J. Exercise and diet, independent of weight loss, improve cardiometabolic risk profile in overweight and obese individuals. Physician Sportsmed. 2011, 39, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Bacon, L.; Aphramor, L. Weight Science: Evaluating the Evidence for a Paradigm Shift. Nutr. J. 2011, 10, 9. [Google Scholar] [CrossRef]
- Warren, J.M.; Smith, N.; Ashwell, M. A structured literature review on the role of mindfulness, mindful eating and intuitive eating in changing eating behaviours: Effectiveness and associated potential mechanisms. Nutr. Res. Rev. 2017, 30, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Corsica, J.; Hood, M.M.; Katterman, S.; Kleinman, B.; Ivan, I. Development of a novel mindfulness and cognitive behavioral intervention for stress-eating: A comparative pilot study. Eat. Behav. 2014, 15, 694–699. [Google Scholar] [CrossRef]
- Jebb, S.A.; Ahern, A.L.; Olson, A.D.; Aston, L.M.; Holzapfel, C.; Stoll, J.; Amann-Gassner, U.; Simpson, A.E.; Fuller, N.R.; Pearson, S.; et al. Primary care referral to a commercial provider for weight loss treatment versus standard care: A randomised controlled trial. Lancet 2011, 378, 1485–1492. [Google Scholar] [CrossRef] [PubMed]
- Metzgar, C.J.; Preston, A.G.; Miller, D.L.; Nickols-Richardson, S.M. Facilitators and barriers to weight loss and weight loss maintenance: A qualitative exploration. J. Hum. Nutr. Diet. 2015, 28, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Stead, M.; Craigie, A.M.; Macleod, M.; McKell, J.; Caswell, S.; Steele, R.J.; Anderson, A.S. Why are some people more successful at lifestyle change than others? Factors associated with successful weight loss in the BeWEL randomised controlled trial of adults at risk of colorectal cancer. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 87. [Google Scholar] [CrossRef] [PubMed]
- Robertson, L.; Smith, M.; Castle, D.; Tannenbaum, D. Using the Internet to enhance the treatment of depression. Australas Psychiatry 2006, 14, 413–417. [Google Scholar] [CrossRef]
- MacLean, P.S.; Wing, R.R.; Davidson, T.; Epstein, L.; Goodpaster, B.; Hall, K.D.; Levin, B.E.; Perri, M.G.; Rolls, B.J.; Rosenbaum, M.; et al. NIH working group report: Innovative research to improve maintenance of weight loss. Obesity 2015, 23, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Hutchings, R. The Impact of Covid-19 on the Use of Digital Technology in the NHS. Available online: https://www.nuffieldtrust.org.uk/research/the-impact-of-covid-19-on-the-use-of-digital-technology-in-the-nhs (accessed on 30 December 2022).
- Bongers, P.; Jansen, A. Emotional Eating Is Not What You Think It Is and Emotional Eating Scales Do Not Measure What You Think They Measure. Front. Psychol. 2016, 7, 1932. [Google Scholar] [CrossRef] [PubMed]
- Censin, J.C.; Peters, S.A.E.; Bovijn, J.; Ferreira, T.; Pulit, S.L.; Mägi, R.; Mahajan, A.; Holmes, M.V.; Lindgren, C.M. Causal relationships between obesity and the leading causes of death in women and men. PLoS Genet. 2019, 15, e1008405. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, J.; Persson, L.O.; Sjöström, L.; Sullivan, M. Psychometric properties and factor structure of the Three-Factor Eating Questionnaire (TFEQ) in obese men and women. Results from the Swedish Obese Subjects (SOS) study. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1715–1725. [Google Scholar] [CrossRef] [PubMed]
- Ozier, A.D.; Kendrick, O.W.; Leeper, J.D.; Knol, L.L.; Perko, M.; Burnham, J. Overweight and obesity are associated with emotion- and stress-related eating as measured by the eating and appraisal due to emotions and stress questionnaire. J. Am. Diet. Assoc. 2008, 108, 49–56. [Google Scholar] [CrossRef]
- El-Sayed, A.M.; Scarborough, P.; Galea, S. Ethnic inequalities in obesity among children and adults in the UK: A systematic review of the literature. Obes. Rev. 2011, 12, e516–e534. [Google Scholar] [CrossRef]
- Barrada, J.R.; van Strien, T.; Cebolla, A. Internal Structure and Measurement Invariance of the Dutch Eating Behavior Questionnaire (DEBQ) in a (Nearly) Representative Dutch Community Sample. Eur. Eat. Disord. Rev. 2016, 24, 503–509. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]





| Population | Intervention | Outcome |
|---|---|---|
| obes * OR overweight OR weight OR BMI OR body mass index OR waist circumference AND Adult * OR over 18 | Mindful * OR mindful eat * OR Emotional Eating OR cognitive behavio * OR Behavio * change OR binge eat * OR comfort eat * OR self-help OR food addiction OR Acceptance and Commitment Therapy OR ACT AND Intervention * OR treatment * | Weight loss OR weight reduction OR lose weight OR eating control |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, J.; Ang, X.Q.; Giles, E.L.; Traviss-Turner, G. Emotional Eating Interventions for Adults Living with Overweight or Obesity: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 2722. https://doi.org/10.3390/ijerph20032722
Smith J, Ang XQ, Giles EL, Traviss-Turner G. Emotional Eating Interventions for Adults Living with Overweight or Obesity: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(3):2722. https://doi.org/10.3390/ijerph20032722
Chicago/Turabian StyleSmith, Jo, Xiao Qi Ang, Emma L. Giles, and Gemma Traviss-Turner. 2023. "Emotional Eating Interventions for Adults Living with Overweight or Obesity: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 3: 2722. https://doi.org/10.3390/ijerph20032722