
Risk Factors Associated with Diarrheal Episodes in an Agricultural Community in Nam Dinh Province, Vietnam: A Prospective Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
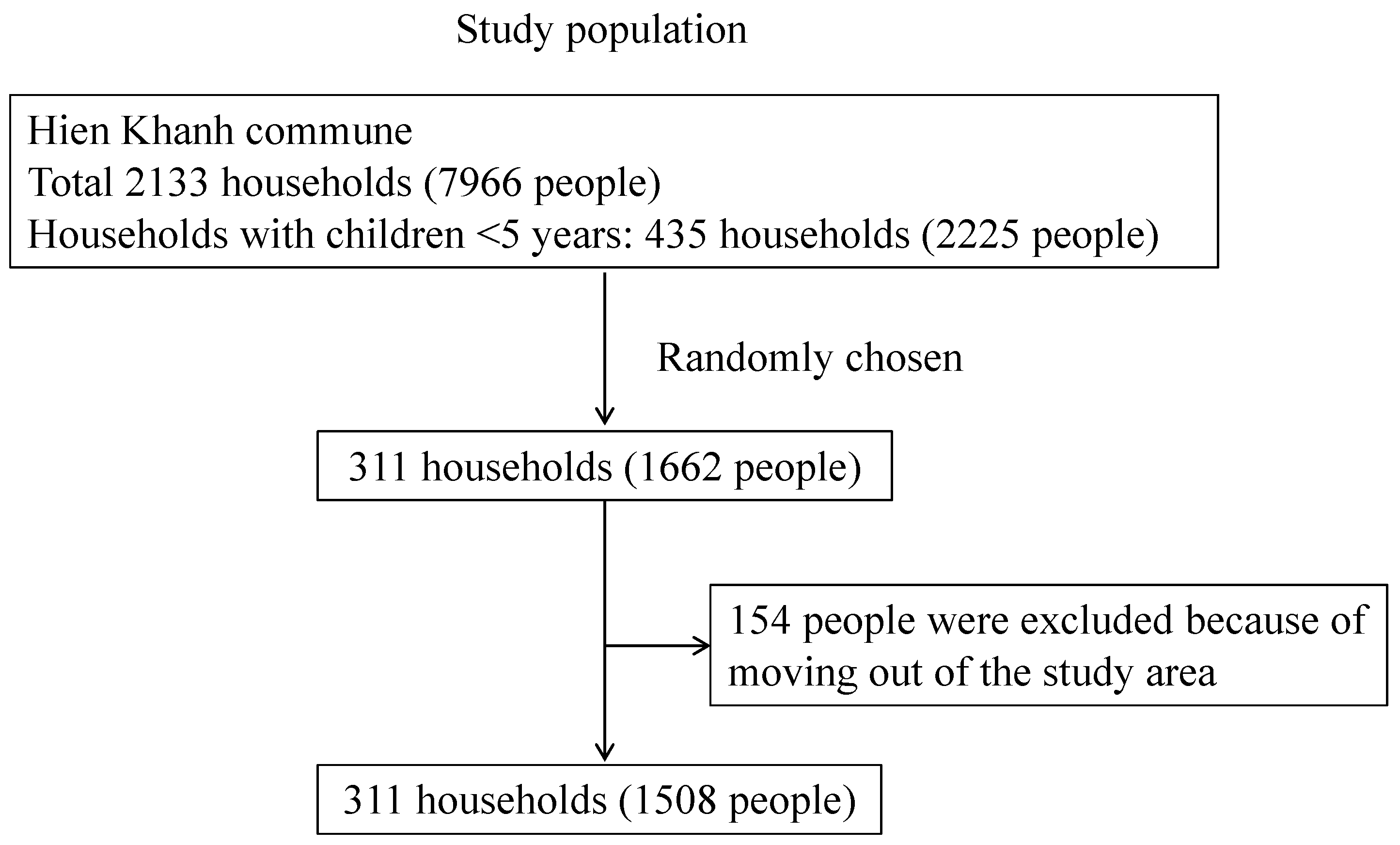
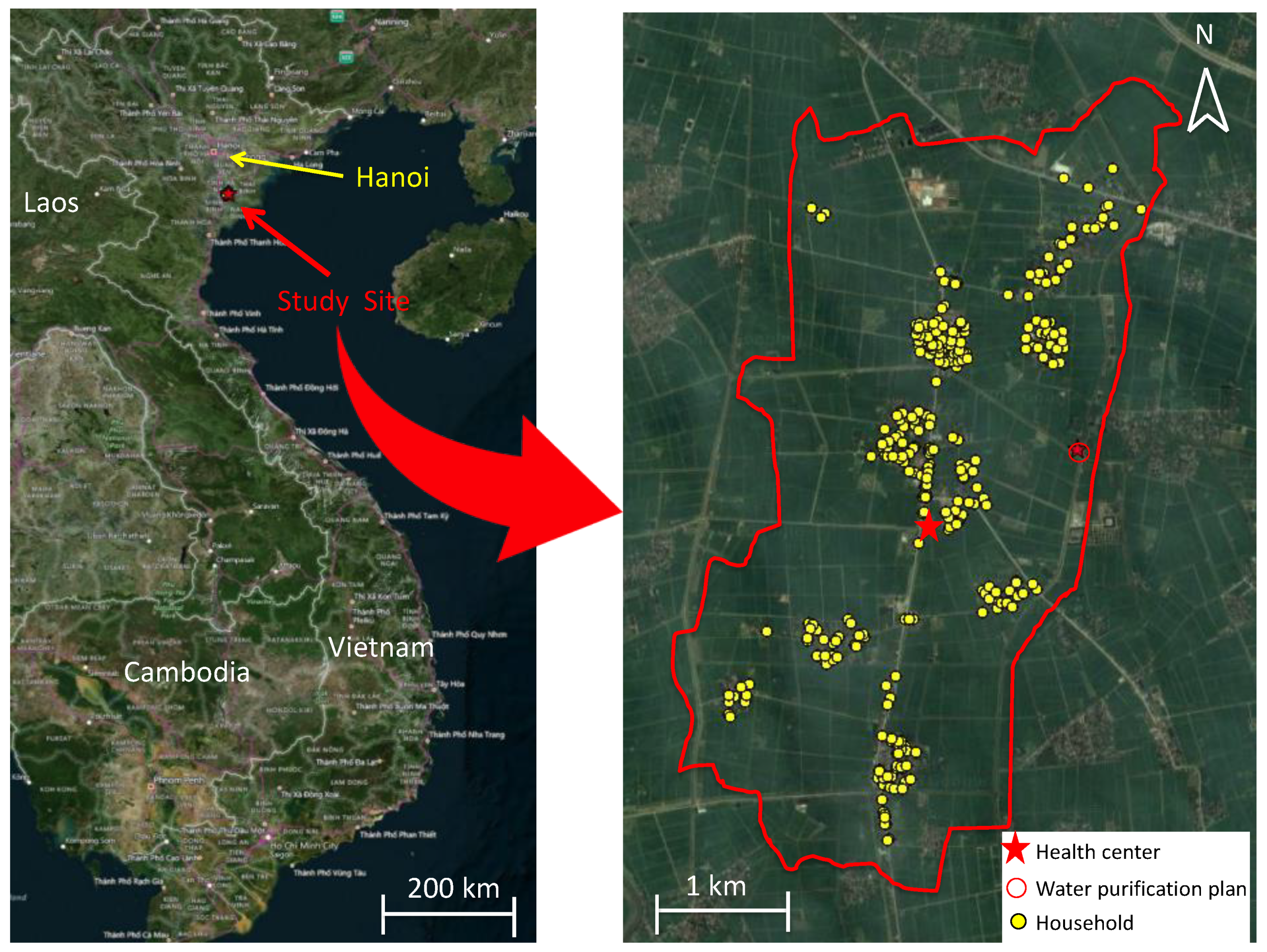
2.1. Study Site and Population
2.2. Research Team
2.3. Participant Inclusion
2.4. Baseline Information through Face-to-Face Interviews Using a Questionnaire
2.5. Global Positioning System (GPS) for Measuring Distances
2.6. Definition of Diarrhea
2.7. Routine Follow-Up for Collecting Data for Diarrhea
2.8. Data Management
2.9. Risk Factor Analysis
3. Results
3.1. Socioeconomic Characteristics of Participants
3.2. Diarrheal Episodes
3.3. Diarrheal Risk Factors
4. Discussion
4.1. Incidence of Recurrent Diarrhea
4.2. Diarrheal Risk Factors
4.3. Potential Risk Factors That Remain Unidentified Following Our Study
4.4. Limitations
4.5. Significance of This Study and Its Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| IRR | Incidence Rate Ratio |
| WPP | Water Purification Plant |
References
- WHO Child Mortality 2019. Levels Trends Child Mortality. 2019, pp. 1–52. Available online: https://www.unicef.org/media/60561/file/UN-IGME-child-mortality-report-2019.pdf (accessed on 13 February 2022).
- Amugsi, D.A.; Aborigo, R.A.; Oduro, A.R.; Asoala, V.; Awine, T.; Amenga-Etego, L. Socio-demographic and environmental determinants of infectious disease morbidity in children under 5 years in Ghana. Glob. Health Action 2015, 8, 29349. [Google Scholar] [CrossRef] [Green Version]
- Akinyemi, Y.C. Exploring the spatio-temporal variation in diarrhoea prevalence in under-five children: The case of Nigeria, 1990–2013. Int. J. Public Health 2019, 64, 1183–1192. [Google Scholar] [CrossRef]
- Tickell, K.D.; Sharmin, R.; Deichsel, E.L.; Lamberti, L.M.; Walson, J.L.; Faruque, A.S.G.; Pavlinac, P.B.; Kotloff, K.L.; Chisti, M.J. The effect of acute malnutrition on enteric pathogens, moderate-to-severe diarrhoea, and associated mortality in the Global Enteric Multicenter Study cohort: A post-hoc analysis. Lancet Glob. Health 2020, 8, e215–e224. [Google Scholar] [CrossRef] [Green Version]
- Dey, N.C.; Parvez, M.; Islam, M.R.; Mistry, S.K.; Levine, D.I. Effectiveness of a community-based water, sanitation, and hygiene (WASH) intervention in reduction of diarrhoea among under-five children: Evidence from a repeated cross-sectional study (2007–2015) in rural Bangladesh. Int. J. Hyg. Environ. Health 2019, 222, 1098–1108. [Google Scholar] [CrossRef]
- Otsuka, Y.; Agestika, L.; Widyarani, N.S.; Yamauchi, T. Risk factors for undernutrition and diarrhea prevalence in an urban slum in Indonesia: Focus on water, sanitation, and hygiene. Am. J. Trop. Med. Hyg. 2019, 100, 727–732. [Google Scholar] [CrossRef] [Green Version]
- Kirby, M.A.; Nagel, C.L.; Rosa, G.; Zambrano, L.D.; Musafiri, S.; Ngirabega, J.d.D.; Thomas, E.A.; Clasen, T. Effects of a large-scale distribution of water filters and natural draft rocket-style cookstoves on diarrhea and acute respiratory infection: A cluster-randomized controlled trial in Western Province, Rwanda. PLoS Med. 2019, 16, e1002812. [Google Scholar] [CrossRef] [Green Version]
- Asoka, G.W.; Thuo, A.D.; Bunyasi, M.M. Effects of Population Growth on Urban Infrastructure and Services: A Case of Eastleigh Neighborhood Nairobi, Kenya. J. Anthropol. Archaeol. 2013, 1, 41–56. [Google Scholar]
- You, D.; Hug, L.; Ejdemyr, S.; Idele, P.; Hogan, D.; Mathers, C.; Gerland, P.; New, J.R.; Alkema, L. Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: A systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. Lancet 2015, 386, 2275–2286. [Google Scholar] [CrossRef]
- Troeger, C.; Forouzanfar, M.; Rao, P.C.; Khalil, I.; Brown, A.; Reiner, R.C.; Fullman, N.; Thompson, R.L.; Abajobir, A.; Ahmed, M.; et al. Estimates of global, regional, and national morbidity, mortality, and aetiologies of diarrhoeal diseases: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 909–948. [Google Scholar] [CrossRef] [Green Version]
- Thompson, C.N.; Phan, M.V.T.; Van Minh Hoang, N.; Van Minh, P.; Vinh, N.T.; Thuy, C.T.; Nga, T.T.T.; Rabaa, M.A.; Duy, P.T.; Dung, T.T.N.; et al. A prospective multi-center observational study of children hospitalized with diarrhea in Ho Chi Minh City, Vietnam. Am. J. Trop. Med. Hyg. 2015, 92, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.V.; Le Van, P.; Le Huy, C.; Weintraub, A. Diarrhea caused by enterotoxigenic Bacteroides fragilis in children less than 5 years of age in Hanoi, Vietnam. Anaerobe 2005, 11, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Hien, B.T.T.; Scheutz, F.; Phung, D.C.; Serichantalergs, O.; Tran, T.H.; Tran, M.T.; Dalsgaard, A. Diarrheagenic Escherichia coli and Shigella strains isolated from children in a hospital case-control study in Hanoi, Vietnam. J. Clin. Microbiol. 2008, 46, 996–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Man, N.; Luan, L.T.; Trach, D.D.; Thanh, N.T.H.; Van Tu, P.; Long, N.T.; Ann, D.D.; Fischer, T.K.; Ivanoff, B.; Gentsch, J.R.; et al. Epidemiological profile and burden of rotavirus diarrhea in Vietnam: 5 Years of sentinel hospital surveillance, 1998–2003. J. Infect. Dis. 2005, 192, 1998–2003. [Google Scholar] [CrossRef]
- Huyen, D.T.T.; Hong, D.T.; Trung, N.T.; Hoa, T.T.N.; Oanh, N.K.; Thang, H.V.; Thao, N.T.T.; Hung, D.M.; Iijima, M.; Fox, K.; et al. Epidemiology of acute diarrhea caused by rotavirus in sentinel surveillance sites of Vietnam, 2012–2015. Vaccine 2018, 36, 7894–7900. [Google Scholar] [CrossRef] [PubMed]
- Thiem, V.D.; Schmidt, W.P.; Suzuki, M.; Tho, L.H.; Yanai, H.; Ariyoshi, K.; Anh, D.D.; Yoshida, L.M. Animal livestock and the risk of hospitalized diarrhoea in children under 5 years in Vietnam. Trop. Med. Int. Health 2012, 17, 613–621. [Google Scholar] [CrossRef] [Green Version]
- Carrique-Mas, J.J.; Bryant, J.E. A review of foodborne bacterial and parasitic zoonoses in Vietnam. Ecohealth 2013, 10, 465–489. [Google Scholar] [CrossRef] [Green Version]
- Iwashita, H.; Sugamoto, T.; Takemura, T.; Tokizawa, A.; Thiem, V.D.; Nguyen, T.H.; Pham, T.D.; Tran, N.L.; Doan, H.T.; Pham, A.H.Q.; et al. Molecular epidemiology of Giardia spp. in northern Vietnam: Potential transmission between animals and humans. Parasite Epidemiol. Control 2020, 12, e00193. [Google Scholar] [CrossRef]
- Genser, B.; Strina, A.; Dos Santos, L.A.; Teles, C.A.; Prado, M.S.; Cairncross, S.; Barreto, M.L. Impact of a city-wide sanitation intervention in a large urban centre on social, environmental and behavioural determinants of childhood diarrhoea: Analysis of two cohort studies. Int. J. Epidemiol. 2008, 37, 831–840. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, C.E. Home Is Where the Health Is: Housing and Adult Height from the Late 19th to the Mid-20th Centuries; European Real Estate Society (ERES), 2018; Available online: https://library.eres.org/eres2018/paperupload/P_20180116123935_653.pdf (accessed on 13 February 2022).
- Budhathoki, S.S.; Bhattachan, M.; Yadav, A.K.; Upadhyaya, P.; Pokharel, P.K. Eco-social and behavioural determinants of diarrhoea in under-five children of Nepal: A framework analysis of the existing literature. Trop. Med. Health 2016, 44, 7. [Google Scholar] [CrossRef] [Green Version]
- Gebru, T.; Taha, M.; Kassahun, W. Risk factors of diarrhoeal disease in under-five children among health extension model and non-model families in Sheko district rural community, Southwest Ethiopia: Comparative cross-sectional study. BMC Public Health 2014, 14, 395. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Regional Office for Europe; Ranson, R.P. Guidelines for Healthy Housing; WHO Regional Office for Europe: Copenhagen Denmark, 1988. [Google Scholar]
- Suzuki, M.; Thiem, V.D.; Yanai, H.; Matsubayashi, T.; Yoshida, L.M.; Tho, L.H.; Minh, T.T.; Anh, D.D.; Kilgore, P.E.; Ariyoshi, K. Association of environmental tobacco smoking exposure with an increased risk of hospital admissions for pneumonia in children under 5 years of age in Vietnam. Thorax 2009, 64, 484–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filmer, D.; Pritchett, L.H. Estimating Wealth Effects Estimating Wealth Effects without Expenditure Data—Or Tears: An Application to Educational Enrollments in States of India. Demography 2001, 38, 115–132. [Google Scholar] [PubMed] [Green Version]
- Larson, P.S.; Minakawa, N.; Dida, G.O.; Njenga, S.M.; Ionides, E.L.; Wilson, M.L. Insecticide-treated net use before and after mass distribution in a fishing community along Lake Victoria, Kenya: Successes and unavoidable pitfalls. Malar. J. 2014, 13, 466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Womack, N.C. Treatment of diarrhea. South. Med. J. 1924, 17, 562–563. [Google Scholar] [CrossRef]
- Kotloff, K.L.; Blackwelder, W.C.; Nasrin, D.; Nataro, J.P.; Farag, T.H.; Van Eijk, A.; Adegbola, R.A.; Alonso, P.L.; Breiman, R.F.; Golam Faruque, A.S.; et al. The Global Enteric Multicenter Study (GEMS) of diarrheal disease in infants and young children in developing countries: Epidemiologic and clinical methods of the case/control study. Clin. Infect. Dis. 2012, 55 (Suppl. S4), S232–S245. [Google Scholar] [CrossRef] [Green Version]
- Bolker, B.; Skaug, H.; Magnusson, A.; Nielsen, A. Getting Started with the glmmADMB Package. 2012. 12. Available online: https://glmmadmb.r-forge.r-project.org/glmmADMB.pdf (accessed on 13 February 2022).
- Zuur, A.; Ieno, E.N.; Walker, N.; Saveliev, A.A.; Smith, G.M. Mixed Effects Models and Extensions in Ecology with R; Springer: New York, NY, USA, 2009; ISBN 0387874585. [Google Scholar]
- Faraway, J.J. Extending the Linear Model with R: Generalized Linear, Mixed Effects and Nonparametric Regression Models; CRC Press: Boca Raton, FL, USA, 2016; ISBN 1498720986. [Google Scholar]
- Aluisio, A.R.; Maroof, Z.; Chandramohan, D.; Bruce, J.; Masher, M.I.; Manaseki-Holland, S.; Ensink, J.H.J. Risk factors associated with recurrent diarrheal illnesses among children in Kabul, Afghanistan: A prospective cohort study. PLoS ONE 2015, 10, e0116342. [Google Scholar] [CrossRef]
- George, C.M.; Perin, J.; De Calani, K.J.N.; Norman, W.R.; Perry, H.; Davis, T.P.; Lindquist, E.D. Risk factors for diarrhea in children under five years of age residing in Peri-urban Communities in Cochabamba, Bolivia. Am. J. Trop. Med. Hyg. 2014, 91, 1190–1196. [Google Scholar] [CrossRef] [Green Version]
- Alelign, T.; Asegidew, W.; Abera, A. A Cross Sectional Study on the Incidence and Risk Factors of Diarrheal Illness among Children Under-five Years of Age in Debre Berhan Town, Ethiopia. J. Health Med. Econ. 2016, 2, 12. [Google Scholar] [CrossRef]
- Trang, D.T.; Hien, B.T.T.; Mølbak, K.; Cam, P.D.; Dalsgaard, A. Epidemiology and aetiology of diarrhoeal diseases in adults engaged in wastewater-fed agriculture and aquaculture in Hanoi, Vietnam. Trop. Med. Int. Health 2007, 12, 23–33. [Google Scholar] [CrossRef]
- Fischer Walker, C.L.; Perin, J.; Aryee, M.J.; Boschi-Pinto, C.; Black, R.E. Diarrhea incidence in low- and middle-income countries in 1990 and 2010: A systematic review. BMC Public Health 2012, 12, 220. [Google Scholar] [CrossRef] [Green Version]
- Pham-Duc, P.; Nguyen-Viet, H.; Hattendorf, J.; Cam, P.D.; Zurbrügg, C.; Zinsstag, J.; Odermatt, P. Diarrhoeal diseases among adult population in an agricultural community Hanam province, Vietnam, with high wastewater and excreta re-use. BMC Public Health 2014, 14, 978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, C.L.F.; Black, R.E. Diarrhoea morbidity and mortality in older children, adolescents, and adults. Epidemiol. Infect. 2010, 138, 1215–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kattula, D.; Francis, M.R.; Kulinkina, A.; Sarkar, R.; Mohan, V.R.; Babji, S.; Ward, H.D.; Kang, G.; Balraj, V.; Naumova, E.N. Environmental predictors of diarrhoeal infection for rural and urban communities in south India in children and adults. Epidemiol. Infect. 2015, 143, 3036–3047. [Google Scholar] [CrossRef] [PubMed]
- Thiam, S.; Diène, A.N.; Fuhrimann, S.; Winkler, M.S.; Sy, I.; Ndione, J.A.; Schindler, C.; Vounatsou, P.; Utzinger, J.; Faye, O. Prevalence of diarrhoea and risk factors among children under five years old in Mbour, Senegal: A cross-sectional study. Infect. Dis. poverty 2017, 6, 43–54. [Google Scholar] [CrossRef] [Green Version]
- Clasen, T.; Schmidt, W.P.; Rabie, T.; Roberts, I.; Cairncross, S. Interventions to improve water quality for preventing diarrhoea: Systematic review and meta-analysis. Br. Med. J. 2007, 334, 782–785. [Google Scholar] [CrossRef] [Green Version]
- Son, P.T.; Voropai, N. The Major Outage in South Vietnam in 2013: The Nature of Blackout, Security Measures and Strategy of National Power System Modernization. In Proceedings of the International Conference on Problem of Critical Structures; 2015; pp. 177–182. Available online: https://isem.irk.ru/upload/medialibrary/842/8427a717228acbec7243f33cd6a82a9e.pdf (accessed on 13 February 2022).
- LeChevallier, M.W.; Gullick, R.W.; Karim, M.R.; Friedman, M.; Funk, J.E. The potential for health risks from intrusion of contaminants into the distribution system from pressure transients. J. Water Health 2003, 1, 3–14. [Google Scholar] [CrossRef]
- Ozdemir, S.; Elliott, M.; Brown, J.; Nam, P.K.; Hien, V.T.; Sobsey, M.D. Rainwater harvesting practices and attitudes in the mekong delta of Vietnam. J. Water Samit. Hyg. Dev. 2011, 1, 171–177. [Google Scholar] [CrossRef]
- Meera, V.; Ahammed, M.M. Water quality of rooftop rainwater harvesting systems: A review. J. Water Supply Res. Technol. 2006, 55, 257–268. [Google Scholar] [CrossRef]
- Ahmed, W.; Huygens, F.; Goonetilleke, A.; Gardner, T. Real-time PCR detection of pathogenic microorganisms in roof-harvested rainwater in Southeast Queensland, Australia. Appl. Environ. Microbiol. 2008, 74, 5490–5496. [Google Scholar] [CrossRef] [Green Version]
- Fewtrell, L.; Kay, D. Microbial quality of rainwater supplies in developed countries: A review. Urban Water J. 2007, 4, 253–260. [Google Scholar] [CrossRef]
- Hamilton, K.; Reyneke, B.; Waso, M.; Clements, T.; Ndlovu, T.; Khan, W.; DiGiovanni, K.; Rakestraw, E.; Montalto, F.; Haas, C.N.; et al. A global review of the microbiological quality and potential health risks associated with roof-harvested rainwater tanks. NPJ Clean Water 2019, 2, 7. [Google Scholar] [CrossRef]
- Yates, T.; Vujcic, J.A.; Joseph, M.L.; Gallandat, K.; Lantagne, D. Efficacy and effectiveness of water, sanitation, and hygiene interventions in emergencies in low-and middle-income countries: A systematic review. Waterlines 2018, 37, 31–65. [Google Scholar] [CrossRef]
- Deichsel, E.L.; Pavlinac, P.B.; Mbori-Ngacha, D.; Walson, J.L.; Maleche-Obimbo, E.; Farquhar, C.; Bosire, R.; John-Stewart, G.C. Maternal Diarrhea and Antibiotic Use are Associated with Increased Risk of Diarrhea among HIV-Exposed, Uninfected Infants in Kenya. Am. J. Trop. Med. Hyg. 2020, 102, 1001. [Google Scholar] [CrossRef] [Green Version]
- Dearden, K.A.; Schott, W.; Crookston, B.T.; Humphries, D.L.; Penny, M.E.; Behrman, J.R. Children with access to improved sanitation but not improved water are at lower risk of stunting compared to children without access: A cohort study in Ethiopia, India, Peru, and Vietnam. BMC Public Health 2017, 17, 110. [Google Scholar] [CrossRef] [Green Version]
- Noguchi, Y.; Nonaka, D.; Kounnavong, S.; Kobayashi, J. Effects of Hand-Washing Facilities with Water and Soap on Diarrhea Incidence among Children under Five Years in Lao People’s Democratic Republic: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 687. [Google Scholar] [CrossRef]
- Jung, Y.T.; Hum, R.J.; Lou, W.; Cheng, Y.-L. Effects of neighbourhood and household sanitation conditions on diarrhea morbidity: Systematic review and meta-analysis. PLoS ONE 2017, 12, e0173808. [Google Scholar] [CrossRef] [Green Version]
- McIntosh, A.C.; Makin, I.; Paw, T.G.; Dhamasiri, C.; Thapan, A.; Rivera, P.; Liemberger, R.; White, M. Urban water supply and sanitation in Southeast Asia: A guide to good practice. 2014. Available online: http://hdl.handle.net/11540/5038 (accessed on 13 February 2022).
- Zambrano, L.D.; Levy, K.; Menezes, N.P.; Freeman, M.C. Human diarrhea infections associated with domestic animal husbandry: A systematic review and meta-analysis. Trans. R. Soc. Trop. Med. Hyg. 2014, 108, 313–325. [Google Scholar] [CrossRef] [Green Version]
- Iwashita, H.; Takemura, T.; Tokizawa, A.; Sugamoto, T.; Thiem, V.D.; Nguyen, T.H.; Pham, T.D.; Pham, A.H.Q.; Doan, H.T.; Tran, N.L. Molecular epidemiology of Cryptosporidium spp. in an agricultural area of northern Vietnam: A community survey. Parasitol. Int. 2021, 83, 102341. [Google Scholar] [CrossRef]
- World Health Organization. Country Case Studies on Primary Health Care: Viet Nam: Improving Equity in Access to Primary Care; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. The Treatment of Diarrhoea: A Manual for Physicians and Other Senior Health Workers; World Health Organization: Geneva, Switzerland, 2005; ISBN 9241593180. [Google Scholar]
- Thompson, C.N.; Zelner, J.L.; Nhu, T.D.H.; Phan, M.V.T.; Hoang Le, P.; Nguyen Thanh, H.; Vu Thuy, D.; Minh Nguyen, N.; Ha Manh, T.; Van Hoang Minh, T.; et al. The impact of environmental and climatic variation on the spatiotemporal trends of hospitalized pediatric diarrhea in Ho Chi Minh City, Vietnam. Health Place 2015, 35, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Oswald, W.E.; Lescano, A.G.; Bern, C.; Calderon, M.M.; Cabrera, L.; Gilman, R.H. Fecal contamination of drinking water within peri-urban households, Lima, Peru. Am. J. Trop. Med. Hyg. 2007, 77, 699–704. [Google Scholar] [CrossRef] [Green Version]
- Darvesh, N.; Das, J.K.; Vaivada, T.; Gaffey, M.F.; Rasanathan, K.; Bhutta, Z.A. Water, sanitation and hygiene interventions for acute childhood diarrhea: A systematic review to provide estimates for the Lives Saved Tool. BMC Public Health 2017, 17 (Suppl. S4), 776. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | No of Households | No of Individuals | % |
|---|---|---|---|
| Sex | |||
| Male | 658 | 43.6 | |
| Female | 850 | 56.4 | |
| Age | |||
| 0–4 | 367 | 24.3 | |
| 5–14 | 234 | 15.5 | |
| 15–49 | 621 | 41.2 | |
| 50–69 | 234 | 15.5 | |
| ≥70 | 52 | 3.4 | |
| Number of children under 5 years in the house | |||
| ≥2 | 82 | 26.4 | |
| <2 | 229 | 73.6 | |
| Household crowding (m2/person) | |||
| <12 m2 | 99 | 536 | 35.5 |
| ≥12 m2 | 212 | 972 | 64.5 |
| Water source for daily use | |||
| Tap water for daily use | |||
| Yes | 289 | 1397 | 92.6 |
| No | 22 | 111 | 7.4 |
| Water truck for daily use | |||
| Yes | 2 | 8 | 0.5 |
| No | 309 | 1500 | 99.5 |
| Tube well/Hand pump for daily use | |||
| Yes | 15 | 84 | 5.6 |
| No | 296 | 1424 | 94.4 |
| Open well for daily use | |||
| Yes | 6 | 32 | 2.1 |
| No | 305 | 1476 | 97.9 |
| Rainwater for daily use | |||
| Yes | 201 | 985 | 65.3 |
| No | 110 | 523 | 34.7 |
| Canal/River for daily use | |||
| Yes | 0 | 0 | 0.0 |
| No | 311 | 1508 | 100.0 |
| Lake/Pond for daily use | |||
| Yes | 3 | 16 | 1.1 |
| No | 308 | 1492 | 98.9 |
| Others for daily use | |||
| Yes | 1 | 5 | 0.3 |
| No | 310 | 1503 | 99.7 |
| Water for drinking | |||
| Tap water | 111 | 530 | 35.1 |
| Rain water | 198 | 971 | 64.4 |
| Other (Mineral, Truck) | 2 | 7 | 0.5 |
| Boiling water | |||
| Yes | 309 | 1500 | 99.5 |
| No | 2 | 8 | 0.5 |
| Distance from WWP (water purification plant) | |||
| <1.5 km | 217 | 1056 | 70.0 |
| ≥1.5 km | 94 | 452 | 30.0 |
| Toilet facility type | |||
| Flush toilet | 244 | 1183 | 78.4 |
| Pit latrine | 55 | 269 | 17.8 |
| Others | 12 | 56 | 3.7 |
| Animals | |||
| Pigs | |||
| Yes | 39 | 206 | 13.7 |
| No | 272 | 1302 | 86.3 |
| Buffalos | |||
| Yes | 5 | 28 | 1.9 |
| No | 306 | 1408 | 98.1 |
| Dogs | |||
| Yes | 215 | 1114 | 73.9 |
| No | 87 | 394 | 26.1 |
| Cattle | |||
| Yes | 30 | 162 | 10.7 |
| No | 281 | 1346 | 89.3 |
| Cats | |||
| Yes | 158 | 786 | 52.1 |
| No | 153 | 722 | 47.9 |
| Chicken or Birds | |||
| Yes | 212 | 1069 | 70.9 |
| No | 99 | 439 | 29.1 |
| Ducks/Geese | |||
| Yes | 50 | 263 | 17.4 |
| No | 261 | 1245 | 82.6 |
| Existence of animal | |||
| Any animal | 277 | 1368 | 90.7 |
| No animal | 34 | 140 | 9.3 |
| Wealth level | |||
| Low | 75 | 340 | 22.5 |
| Middle | 186 | 901 | 59.7 |
| High | 50 | 267 | 17.7 |
| Individuals without Diarrhea | Individuals with Diarrhea | Cumulative Episodes of Diarrhea | Person-Years of Observation | Diarrhea Episodes/Person per Year (95% CI) | Incidence Rate Ratio (IRR) (95% CI) | p Value | |
|---|---|---|---|---|---|---|---|
| Sex | |||||||
| Male | 423 | 235 | 319 | 681.4 | 0.47 (0.41–0.52) | 1 | |
| Female | 513 | 337 | 472 | 880.3 | 0.54 (0.48–0.59) | 1.11 (0.95–1.28) | 0.19 |
| Age | |||||||
| 0–4 | 168 | 199 | 283 | 380.1 | 0.81 (0.71–0.91) | 1.79 (1.52–2.11) | <0.0001 * |
| 5–14 | 153 | 81 | 92 | 242.3 | 0.43 (0.34–0.51) | 0.99 (0.79–1.26) | 0.95 |
| 15–49 | 406 | 215 | 308 | 643.1 | 0.44 (0.39–0.49) | 1 | |
| 50–69 | 162 | 72 | 103 | 242.3 | 0.38 (0.30–0.46) | 0.89 (0.69–1.14) | 0.35 |
| ≥70 | 47 | 5 | 5 | 53.9 | 0.09 (0.01–0.17) | 0.24 (0.10–0.59) | 0.002 * |
| Household crowding (m2/person) | |||||||
| <12 m2 | 335 | 201 | 278 | 555.1 | 0.50 (0.43–0.57) | 0.95 (0.73–1.22) | 0.66 |
| ≥12 m2 | 601 | 371 | 513 | 1006.6 | 0.51 (0.46–0.56) | 1 | |
| Tap water for daily use | |||||||
| Yes | 855 | 542 | 750 | 1446.8 | 0.52 (0.48–0.56) | 1.59 (0.97–2.62) | 0.07 |
| No | 81 | 30 | 41 | 115.0 | 0.36 (0.23–0.49) | 1 | |
| Water truck for daily use | |||||||
| Yes | 4 | 4 | 7 | 8.3 | 0.84 (0.05–1.64) | 1.77 (0.45–6.98) | 0.41 |
| No | 932 | 568 | 784 | 1553.4 | 0.50 (0.47–0.54) | 1 | |
| Tube well/Hand pump for daily use | |||||||
| Yes | 41 | 43 | 61 | 87.0 | 0.70 (0.52–0.88) | 1.53 (0.93–2.53) | 0.10 |
| No | 895 | 529 | 730 | 1474.7 | 0.50 (0.45–0.54) | 1 | |
| Open well for daily use | |||||||
| Yes | 18 | 14 | 20 | 33.1 | 0.60 (0.31–0.89) | 1.17 (0.51–2.66) | 0.71 |
| No | 918 | 558 | 771 | 1528.6 | 0.50 (0.46–0.54) | 1 | |
| Rainwater for daily use | |||||||
| Yes | 657 | 328 | 453 | 1020.1 | 0.44 (0.40–0.49) | 0.67 (0.53–0.85) | 0.001 * |
| No | 279 | 244 | 338 | 541.6 | 0.62 (0.55–0.69) | 1 | |
| Lake/Pond for daily use | |||||||
| Yes | 12 | 4 | 8 | 16.46 | 0.48 (0.00–1.01) | 0.89 (0.26–2.97) | 0.84 |
| No | 924 | 568 | 783 | 1534.6 | 0.51 (0.47–0.55) | 1 | |
| Water for drinking | |||||||
| Tap water | 279 | 251 | 342 | 548.9 | 0.62 (0.56–0.69) | 1.54 (1.21–1.95) | 0.0004 * |
| Rainwater | 656 | 315 | 442 | 1005.6 | 0.44 (0.39–0.49) | 1 | |
| Others (Mineral, Truck) | 1 | 6 | 7 | 7.2 | 0.97 (0.45–1.48) | 2.71 (0.73–10.14) | 0.14 |
| Boiling water | |||||||
| Yes | 935 | 565 | 781 | 1553.4 | 0.50 (0.46–0.54) | 0.41 (0.13–1.29) | 0.13 |
| No | 1 | 7 | 10 | 8.3 | 1.21 (0.64–1.78) | 1 | |
| Distance from WPP (water purification plant) | |||||||
| <1.5 km | 624 | 432 | 605 | 1093.6 | 0.55 (0.50–0.60) | 1.43 (1.10–1.86) | 0.01 * |
| ≥1.5 km | 312 | 140 | 186 | 468.1 | 0.40 (0.33–0.46) | 1 | |
| Toilet facility type | |||||||
| Flush toilet | 765 | 418 | 575 | 1225.1 | 0.47 (0.43–0.51) | 0.69 (0.51–0.92) | 0.01 * |
| Pit latrine | 145 | 124 | 171 | 278.6 | 0.61 (0.52–0.71) | 1 | |
| Others | 26 | 30 | 45 | 58.0 | 0.78 (0.51–1.04) | 1.21 (0.66–2.22) | 0.54 |
| Animal husbandry: Pigs | |||||||
| Yes | 130 | 76 | 110 | 213.3 | 0.52 (0.40–0.63) | 1.04 (0.73–1.48) | 0.82 |
| No | 806 | 496 | 681 | 1348.4 | 0.51 (0.46–0.55) | 1 | |
| Animal husbandry: Buffalos | |||||||
| Yes | 14 | 14 | 16 | 29.0 | 0.55 (0.31–0.79) | 1.20 (0.50–2.90) | 0.69 |
| No | 922 | 558 | 775 | 1532.7 | 0.51 (0.47–0.55) | 1 | |
| Animal husbandry: Dogs | |||||||
| Yes | 699 | 415 | 568 | 1153.7 | 0.49 (0.45–0.54) | 0.85 (0.66–1.11) | 0.24 |
| No | 237 | 157 | 223 | 408.0 | 0.55 (0.47–0.63) | 1 | |
| Animal husbandry: Cattle | |||||||
| Yes | 90 | 72 | 89 | 167.8 | 0.53 (0.43–0.63) | 1.10 (0.75–1.62) | 0.63 |
| No | 846 | 500 | 702 | 1393.9 | 0.50 (0.46–0.55) | 1 | |
| Animal husbandry: Cats | |||||||
| Yes | 505 | 281 | 373 | 814.0 | 0.46 (0.41–0.51) | 0.86 (0.68–1.08) | 0.20 |
| No | 431 | 291 | 418 | 747.7 | 0.56 (0.50–0.62) | 1 | |
| Animal husbandry: Chicken or Birds | |||||||
| Yes | 679 | 390 | 526 | 1107.1 | 0.48 (0.43–0.52) | 0.86 (0.66–1.10) | 0.23 |
| No | 257 | 182 | 265 | 454.6 | 0.58 (0.50–0.67) | 1 | |
| Animal husbandry: Ducks/Geese | |||||||
| Yes | 170 | 93 | 121 | 272.4 | 0.44 (0.36–0.53) | 0.86 (0.63–1.19) | 0.38 |
| No | 766 | 479 | 670 | 1289.3 | 0.52 (0.48–0.56) | 1 | |
| Animal husbandry: Existence of animals | |||||||
| Any animal | 861 | 507 | 704 | 1416.7 | 0.50 (0.46–0.54) | 1.31 (0.89–1.89) | 0.17 |
| No animal | 75 | 65 | 87 | 145.0 | 0.60 (0.48–0.72) | 1 | |
| Wealth level | |||||||
| Low | 376 | 210 | 305 | 606.9 | 0.50 (0.44–0.57) | 1 | |
| Middle | 261 | 163 | 223 | 439.1 | 0.51 (0.43–0.58) | 1.03 (0.77–1.38) | 0.83 |
| High | 299 | 199 | 263 | 515.8 | 0.51 (0.45–0.57) | 1.06 (0.80–1.40) | 0.71 |
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| Adjusted Incidence Rate Ratio (IRR) (95% CI) | p Value | Adjusted Incidence Rate Ratio (IRR) (95% CI) | p Value | |
| Age | ||||
| 0–4 | 1.81 (1.54–2.14) | <0.0001 * | 1.81 (1.54–2.14) | <0.0001 * |
| 5–14 | 0.99 (0.78–1.25) | 0.90 | 0.99 (0.78–1.25) | 0.92 |
| 15–49 | 1 | 1 | ||
| 50–69 | 0.92 (0.72–1.17) | 0.48 | 0.91 (0.71–1.17) | 0.47 |
| ≥70 | 0.24 (0.10–0.59) | 0.002 * | 0.24 (0.10–0.59) | 0.002 * |
| Water source: Tap water for daily use | ||||
| Yes | 1.90 (1.16–3.09) | 0.01 * | 1.81 (1.10–2.96) | 0.02 * |
| No | 1 | 1 | ||
| Water source: Tube well/Hand pump for daily use | ||||
| Yes | 1.55 (0.98–2.45) | 0.06 | 1.55 (0.98–2.46) | 0.06 |
| No | 1 | 1 | ||
| Water source: Rainwater for daily use | ||||
| Yes | 0.71 (0.56–0.89) | 0.004 * | ||
| No | 1 | |||
| Water source for drinking | ||||
| Tap water | 1.44 (1.14–1.81) | 0.002 * | ||
| Rainwater | 1 | |||
| Others | 1.44 (0.42–4.98) | 0.57 | ||
| Boiling water | ||||
| Yes | 0.41 (0.13–1.29) | 0.13 | 0.41 (0.13–1.29) | 0.13 |
| No | 1 | 1 | ||
| Distance from the WPP | ||||
| <1.5 km | 1.62 (1.26–2.08) | 0.0002 * | 1.62 (1.26–2.08) | 0.0002 * |
| ≥1.5 km | 1 | 1 | ||
| Toilet facility type | ||||
| Flush toilet | 0.64 (0.48–0.85) | 0.002 * | 0.66 (0.49–0.88) | 0.004 * |
| Pit latrine | 1 | 1 | ||
| Others | 1.05 (0.59–1.85) | 0.88 | 1.12 (0.63–1.98) | 0.71 |
| Animal husbandry: Cats | ||||
| Yes | 0.85 (0.68–1.06) | 0.14 | 0.84 (0.67–1.05) | 0.12 |
| No | 1 | 1 | ||
| AIC | 2684.0 | 2684.7 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwashita, H.; Tokizawa, A.; Thiem, V.D.; Takemura, T.; Nguyen, T.H.; Doan, H.T.; Pham, A.H.Q.; Tran, N.L.; Yamashiro, T. Risk Factors Associated with Diarrheal Episodes in an Agricultural Community in Nam Dinh Province, Vietnam: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 2456. https://doi.org/10.3390/ijerph19042456
Iwashita H, Tokizawa A, Thiem VD, Takemura T, Nguyen TH, Doan HT, Pham AHQ, Tran NL, Yamashiro T. Risk Factors Associated with Diarrheal Episodes in an Agricultural Community in Nam Dinh Province, Vietnam: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(4):2456. https://doi.org/10.3390/ijerph19042456
Chicago/Turabian StyleIwashita, Hanako, Asako Tokizawa, Vu Dinh Thiem, Taichiro Takemura, Tuan Hai Nguyen, Hang Thi Doan, Anh Hong Quynh Pham, Na Ly Tran, and Tetsu Yamashiro. 2022. "Risk Factors Associated with Diarrheal Episodes in an Agricultural Community in Nam Dinh Province, Vietnam: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 19, no. 4: 2456. https://doi.org/10.3390/ijerph19042456